| SKULL BASE REGION | Jugular foramen |
| HISTOPATHOLOGY | N/A |
| PRIOR SURGICAL RESECTION | No |
| PERTINENT LABORATORY FINDINGS | None |
Case description
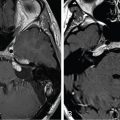
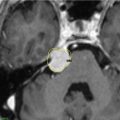
The patient is a 38-year-old female who was evaluated after 3 years of nonspecific disequilibrium and pulsatile tinnitus and was found to have a right jugular foramen mass consistent with schwannoma ( Figure 10.52.1 ). Examination revealed normal cranial nerve function, including normal hearing. Given her age, the location and size of the tumor, and normal cranial nerve function, the decision was made to proceed with stereotactic radiosurgery (SRS) ( Figure 10.52.2 ).
| Radiosurgery Machine | Gamma Knife |
| Radiosurgery Dose (Gy) | 14, at the 50% isodose line |
| Number of Fractions | 1 |

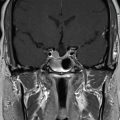
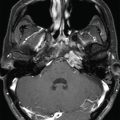
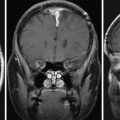
A. Initial MRI 1 month prior to stereotactic radiosurgery (SRS): Axial T1-weighted image with gadolinium showing a heterogeneously enhancing mass of the jugular foramen. B. Initial MRI 1 month prior to SRS: Coronal T1-weighted image with gadolinium showing inferior tumor extension into the neck. C. Initial CT scan 1 month prior to SRS: Axial non-contrasted image demonstrating smooth enlargement of the jugular foramen and minimal bony erosion.

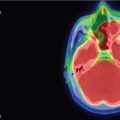
Imaging of the treatment plan. Yellow line, 50% isodose; outer green line, 30% isodose; inner green line, 80% isodose; blue, cochlea outline.
| Critical Structure | Dose Tolerance |
|---|---|
| Brainstem | 15 Gy maximum point dose |
| Internal carotid artery in canal | Unknown dose tolerance |
| Cochlea | 4 Gy maximum point dose (extrapolated from vestibular schwannoma literature) |
| Lower cranial nerves in foramen | Unknown dose tolerance |
| Side Effects/Complications | Frequency |
|---|---|
| Deteriorating lower cranial neuropathy | 3%–7.5% , |
| New lower cranial nerve neuropathy | 15%–17% at 5 years , |
| Malignant transformation (or malignancy within SRS field) |
|
| Internal carotid artery stenosis | Unknown in jugular schwannoma literature. Paraganglioma literature suggests risk of clinically significant carotid stenosis is negligible |
Related posts:
 Esthesioneuroblastoma – delayed postoperative radiosurgery for recurrence at long-term
Esthesioneuroblastoma – delayed postoperative radiosurgery for recurrence at long-term
 Null cell – delayed postoperative radiosurgery for growing perioptic residual
Null cell – delayed postoperative radiosurgery for growing perioptic residual
 Chondrosarcoma – definitive radiosurgery after subtotal resections
Chondrosarcoma – definitive radiosurgery after subtotal resections
 Large vestibular schwannoma – delayed postoperative radiosurgery for growing residual
Large vestibular schwannoma – delayed postoperative radiosurgery for growing residual
 Trigeminal neuralgia due to petroclival meningioma – upfront radiosurgery
Trigeminal neuralgia due to petroclival meningioma – upfront radiosurgery
 Superior sagittal sinus meningioma – delayed postoperative, multisession radiosurgery for growing residual
Superior sagittal sinus meningioma – delayed postoperative, multisession radiosurgery for growing residual
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


