CHAPTER 40 Labyrinthitis Ossifications
Epidemiology
Also termed “ossifying labyrinthitis” and “labyrinthine ossification,” labyrinthitis ossificans (LO) refers to the chronic pathologic ossification of the labyrinth and cochlea from an infectious, inflammatory, traumatic, or surgical insult. Although the most common cause of LO is suppurative bacterial labyrinthitis, other causes include viral labyrinthitis, autoimmune inner ear disease, advanced otosclerosis, labyrinthine artery occlusion, leukemia, and temporal bone tumors. Since bacterial labyrinthitis primarily involves children, LO is observed mainly in the pediatric population.
Clinical Features
Due to involvement of the labyrinth, bilateral sensorineural hearing loss is the most common clinical presentation of LO. Patients with LO may also suffer from vertigo of variable severity, sometimes requiring labyrinthectomy. There is gradual deterioration of hearing after the inciting event, which can be infectious meningitis, trauma, or surgery.
Pathology
Suppurative infection of the membranous labyrinth causes a cascade of inflammatory reactions that result in initial fibrosis followed by ossification. Bone formation can be seen as early as 2 months following the inciting event. On gross pathologic examination, there is new bone formation noted in the membranous labyrinth. Microscopic examination reveals fibroblast proliferation in the initial stages followed by prominent osteoblastic activity. Scala tympani of the basal turn of the cochlea is the most frequently involved area of ossification in LO resulting from any cause.
Treatment
Cochlear implantation is used for treating the sensorineural loss due to LO. It is important to recognize bilateral cochlear LO because bilaterality is a detriment to cochlear implantation.
Imaging Findings
CT
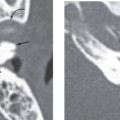
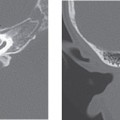
Nonenhanced high-resolution computed tomography (CT) of the temporal bone reveals a spectrum of findings in LO varying from hazy areas of increased density resulting from fibrosis within the fluid spaces of the membranous labyrinth to focal or complete obliteration of the fluid spaces by new bone formation. This can result in a complete “white-out” appearance of the membranous labyrinth. The modiolus can appear prominent. Contrast-enhanced CT has no role in the diagnosis or characterization of LO (Fig. 40-1
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


