Cirrhotic liver shows a small right lobe. The caudate lobe and lateral segment of the left lobe are enlarged. The margins of the liver are irregular. Hepatic parenchyma is heterogeneous because of fatty infiltration, fibrosis, and regenerative nodules.
The hepatic vessels may be diffcult to see because of compression by fibrosis.
Findings of portal hypertension are often seen.
Differentiation of regenerative nodules from hepatocellular carcinoma may be diffcult by imaging techniques.
Diffuse involvement of the liver in neuroblastoma stage 4 and 4S: “salt and pepper” pattern (good prognosis).
Compression and distortion of normal vascular anatomy.
Acute hepatitis
Nonhomogeneous echo pattern; hepatomegaly; periportal edema with increased periportal echogenicity.
Thickening of gallbladder wall; portal lymph-adenopathy.
Chronic granulomatous disease
Multiple, poorly defined hepatic abscesses.
Lesions may resolve or calcify with treatment.
Recurrent infections of the lung, bones, lymph nodes, or liver.
Diffuse hemangioma
Near-total replacement of hepatic parenchyma by the tumor. Below the celiac axis, the aorta has a marked decrease in caliber as a result of increased hepatic arterial flow.
In diffuse hemangiomas, cardiac failure secondary to high volume shunting, hypothyroidism, fulminant hepatic failure, abdominal compartment syndrome, and even death may occur.
Irradiated liver
In the chronic stage (after 6 wks), the liver is typically small, contracted, and fibrotic.
Liver transplantation
A periportal area of low echogenicity (dilatation of lymphatic channels) is often seen after transplantation. On computed tomography (CT) peri-portal edema is seen as a central or peripheral low-attenuation area and has been called the “periportal collar” sign.
Chronic congestion in cardiac disease
Ultrasound (US): echogenic liver parenchyma.
The hepatic veins adjacent to the vena cava are often enlarged.
Chemotherapy
US: enlarged liver, echogenic in comparison to the normal renal parenchyma due to steatosis. Differential diagnosis (DD): veno-occlusive disease, excluded by Doppler.
Toxic effect of chemotherapy.
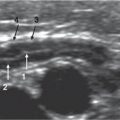
Fig. 2.1 Liver cirrhosis. High-resolution transverse US of the left hepatic lobe. A heterogeneous liver parenchyma with ill-defined hyperechoic nodules is seen in this 13-year-old boy with Wilson disease and portal hypertension.Fig. 2.2 Biliary atresia. Transverse US of the right hepatic lobe. Hepatic parenchyma is heterogeneous with hyperechoic areas related to portal spaces.Fig. 2.3 Neuroblastoma metastases (stage 4S). T2-weighted MRI shows confined left primary adrenal neuroblastoma (N) and hepatomegaly with practically complete liver infiltration by metastases.
Table 2.2 Homogeneous liver parenchyma
Diagnosis
Findings
Comments
Diffuse fatty infiltration
US: Increased parenchymal echogenicity. Appreciation and evaluation of the hepatic echotexture is often diffcult and operator-dependent.
The degree of acoustic attenuation is easier evaluated when comparing the liver to the healthy kidney. An enlarged liver suggests fatty change. Further work-up: magnetic resonance imaging (MRI) in obese patients and biopsy.
Fatty liver in obesity, hyperalimentation with high fat content, hepatitis, long-term steroid therapy, Cushing disease, diabetes mellitus, severe malabsorption, protein-deficiency malnutrition, toxic and drug reactions, hyperlipidemia, familial hyperlipoproteinemia, cystic fibrosis, Reye syndrome, Wilson disease, glycogen storage disease.
Hyperechoic portal spaces related to diffuse hypoechogenicity.
Related to fasting and/or vomiting; reverses after meals.
Edema in acute hepatitis
Hepatomegaly and lymphatic periportal edema.
Progressive gallbladder wall thickening or small amounts of clear fluid in the perihepatic space and in the gallbladder fossa. Frequently enlarged lymph nodes in the hepatic ilium.
Acute congestion in cardiac disease
US: hypoechoic liver parenchyma.
Dilated hepatic veins.
Iron deposition in the liver
MRI is the best imaging modality. Marked decrease in signal intensity on T2- and T1-weighted images.
Either in the hepatocytes (primary hemochromatosis, cirrhosis) or in the reticuloendothelial cells (hemosiderosis).
Fig. 2.4a, b Starry-sky liver. (a) US of liver (right) and spleen (left) showing a homogeneous hypoechoic parenchyma with relatively hyperechoic portal spaces. The hypoechogenicity of liver has been related with prolonged fasting and/or vomiting. (b) Transverse image of liver.
Large, solid mass with cystic areas (hemorrhage). Manganese-enhanced MRI may be used for increasing detection of small satellite lesions and elucidating tumoral or nontumoral thrombus.
Mean age is 0–3 y. Most common primary malignant hepatic tumor (50%).
Possible venous involvement (intravascular solid material, venous encasement).
Calcifications (40%).
Hepatocellular carcinoma
US: Sometimes thin hypoechoic halo (tumor capsule) and hypoechoic areas secondary to necrosis. Rare calcifications (frequent in fibrolamellar scar).
CT or MRI: central scar on fibrolamellar subtype.
Mean age is 12–14 y. Underlying liver disease (50%): tyrosinemia, biliary atresia, familial cholestasis, Alagille syndrome, glycogen storage disease type 1, chronic hepatitis.
Growth patterns: solitary, multifocal, or diffuse.
Well delineated by a fibrotic pseudocapsule. Multi-septated cystic or inhomogeneous solid appearance. Discordance between US imaging (heterogeneous solid mass) and CT or MRI (cystic appearance due to myxomatous tissue).
Mean age is 8–12 y. Most frequent pediatric hepatic sarcoma, though uncommon (5%).
Growth patterns: solitary, multifocal, diffuse, perihepatic, or periportal infiltration (rare but characteristic). Hepatomegaly (not necessarily due to lymphomatous infiltration).
Mean age is 2–16 y. Twelve percent of lymphomas affect the liver. Burkitt lymphoma most frequent. Posttransplantation lymphoproliferative disease: Epstein-Barr-virus–related.
Focal: Hepatic form of the cutaneous rapidly involuting congenital hemangioma (RICH). Fast spontaneous involution. Multiple hepatic lesions (multifocal) or near-total replacement of hepatic parenchyma (diffuse).
Neonates and infants, some diagnosed prenatally. Most common benign pediatric liver tumor (50%).
In diffuse hemangiomas, cardiac failure, hypothyroidism, and fulminant hepatic failure may occur.
Twenty to forty percent have skin hemangiomas. glucose transporter (GLUT)-1 positive in diffuse forms and GLUT-1 negative in focal forms.
US: mass with echogenicity similar to the liver. Central scar in 33% of the cases. T2 with ferumoxide: lesion decreased signal except scar, manganese-enhancement.
Unusual, 5% of all benign hepatic tumors. Associations: type I and type VI glycogen storage disease, Hurler syndrome, galactosemia.
Hepatic adenoma
Imaging depends on the attenuation of the surrounding liver.
Low attenuation (fat, old hemorrhage) or high attenuation (recent hemorrhage, glycogen, surrounding fatty liver).
No uptake of superparamagnetic iron oxide particles.
Associations: intake of androgens, type I glycogen storage disease, human immunodeficiency virus infection, and oral contraceptives.
Chocolate-like content with leukocytes or amebae (may only be seen in abscess wall). Peripherally located (near or in contact to Glisson capsule). Peripheral “halo.” Doppler: no prominent peripheral vascularization (differential finding compared to pyogenic abscess).
In 3%–7% of patients with Entamoeba histolytica infection. More frequent in patients younger than 3 y.
Imaging: hyperechoic on US, homogenous low-attenuation lesion (less than —20 Hounsfield units [HU]) on CT, and high signal intensity on in-phase, drop in signal intensity on out-phase T1-weighted and iso- or hyperintense on T2-weighted MRI.
Rare in children.
Fig. 2.5a–d Mixed hepatoblastoma. (a) Transverse US shows that calcifications (arrows) and cystic necrotic areas (arrowhead) are dominant features. Axial T2-weighted MRI (b) and T1-weighted MRI (c) show right lobe and segment 4 mass. Note areas of increased signal intensity: hemorrhage (arrow) and hypointense bands (fibrous septations; arrowheads). (d) T1-weighted manganese-enhanced MRI. A 4-year-old boy with resected segment 6 hepatoblastoma. A postoperative inferior vena cava (IVC) thrombus was detected (arrows). Manganese enhancement of the thrombus (equal to liver) confirms its tumoral nature.Fig. 2.6a–c Undifferentiated embryonal sarcoma in a 12-year-old boy. (a) Doppler US shows avascular, heterogeneous, apparently solid mass. (b) T2-weighted MRI shows septated, heterogeneous, but predominately cystic sarcoma. (c) Gadolinium-enhanced T1-weighted MRI shows enhancing parietal nodules corresponded to solid portions (arrow).Fig. 2.7a, b Angiosarcoma in a 9-year-old boy. (a) Transverse US shows poorly defined heterogeneous but mainly hyperechoic lesion (arrows). (b) T2-weighted MRI.Fig. 2.8a, b Multicentric Burkitt lymphoma in a 10-year-old boy with abdominal pain due to ileocolic intussusception. (a) US and (b) coronal contrast-enhanced CT show multiple, homogeneous, lowechogenicity/attenuation nodules (arrowheads). The presence of hepatic nodules and the patient’s age serve to rule out lymphoma.Fig. 2.9 Posttransplantation lymphoproliferative disease. Contrast-enhanced CT shows multinodular, partially enhanced hepatic lymphoma 2 years after liver transplantation in an 8-year-old girl.Fig. 2.10a–c Multiple hemangiomas. (a) Transverse US shows multiple hypoechoic lesions, with central echoes, corresponding to vessels (arrow). (b) Doppler US shows vascular rim along the edges of the tumor, with little flow within the tumor itself. (c) Early postcontrast CT: peripheral enhancement of multiple diffusely distributed nodules.Fig. 2.11a, b Focal nodular hyperplasia. (a) Longitudinal US shows well-defined, practically isoechoic in the right lobe of the liver (cursors). (b) Manganese-enhanced T1-weighted MRI shows lesion (arrows) enhancement (similar to the liver parenchyma) demonstrating hepatocellular origin.Fig. 2.12a, b Pyogenic abscess in a 6-year-old with liver transplantation. (a) US: heterogeneous, encapsulated fluid collection containing gas (arrows). (b) Contrast-enhanced CT obtained during percutaneous drainage (arrow) confirmed collection was an abscess.Fig. 2.13 Hepatosplenic candidiasis in a 3-year-old with acute lymphoblastic leukemia and neutropenia. US scan shows multiple hypoechoic hepatic nodules (arrowheads; most frequent US pattern).Fig. 2.14 Focal fatty liver. Transverse US shows well-marginated hyperechogenicity of liver parenchyma that affects lateral right hepatic segments (arrows), with the rest of the liver preserved.Fig. 2.15 Angiomyolipoma in a 17-year-old girl with tuberous sclerosis. T1-weighted in-phase MRI shows small hyperintense lesion in the left lateral segment (arrow).
Table 2.4 Cystic lesions
Diagnosis
Findings
Comments
Normal variants: loops of small bowel in the porta hepatis, caudate lobe, Riedel lobe
If a loop of bowel is suspected in the porta hepatis, US must be performed.
In case of doubt, CT after oral contrast administration may be necessary.
Well-delineated small cyst anechoic or with fine echoes (due to mucoid content) on US and hypoattenuating or isoattenuating relative to surrounding liver parenchyma on CT.
MRI: hyperintense on T2-weighted, variable on T1-weighted (due to variable content).
Solitary cyst. Congenital (embryonic foregut remnant in the liver).
Often < 3 cm and located in segment 4. Rarely, malignant transformation through squamous metaplasia.
Multiseptated cystic mass, although a single dominant cyst may be seen.
Echogenic material within the cyst fluid secondary to blood. Doppler: avascular. On MRI, signal intensity may vary depending on stromal, protein, or hemorrhage contents.
Patients under 2 y. Hamartoma is the second most common benign hepatic tumor (22%).
Predominantly located in the right hepatic lobe.
Posttraumatic hematomas or bilomas
Intrahepatic bilomas usually present on US or CT as intrahepatic peripheral cystic lesions that communicate with the bile duct.
Image-guided aspiration of a fluid collection can be necessary to determine composition.
Mucocele
On US, mucoceles appear as cystic masses near the porta hepatis.
These abnormalities are readily seen as cystic structures on MR cholangiography.
Cystic duct remnant mucocele is an uncommon complication of liver transplant that occurs when the donor cystic duct remnant becomes distended with mucus.
Post-Kasai procedure (hepatojejunostomy)
The jejunal loop is anastomosed with the bile ducts in the porta hepatis. The anastomosis may appear cystic.
Choledochal cysts
Hepatobiliary. US and radionuclide studies usually suggest the correct diagnosis, which can be confirmed by MR cholangiography. Frequently, the intrahepatic ducts are normal. Sludge or stones may be identified within the dilated ducts.
The most common form (80%–90% of cases) is Todani type I (dilatation of the common bile duct).
A characteristic triad of abdominal pain, obstructive jaundice, and fever is only seen in a minority of patients.
Caroli disease
Recognition of the connection of the ectatic ducts with one another and with the rest of the ductal system is critical in distinguishing Caroli disease from polycystic liver disease.
Central dot sign.
Represents segmental or diffuse nonobstructive dilatation of the intrahepatic ducts.
Polycystic liver disease
Hepatobiliary cysts may be intrahepatic or peribiliary.
Occasionally, echogenic debris can be seen if hemorrhage has occurred.
Posttraumatic cysts and posthepatic infarct cysts (liver transplant)
In late phase posthepatic infarct, cystic image is similar to posttraumatic or echinococcal cysts, mainly in the periphery of the liver. Usually after hepatic artery stenosis or thrombosis in transplanted liver.
In posttraumatic cysts, the clinical history of trauma is the diagnostic key.
Fig. 2.16a, b Echinococcosis. (a) Longitudinal oblique US: single lobular cystic lesion with thin wall, through transmission, and internal daughter cysts (type II) (arrow). (b) Coronal T2-weighted MRI: hyperintense cysts with internal septa (arrowhead).Fig. 2.17a–c Ciliated foregut cyst in a 7-year-old girl. (a) Transverse US shows irregular, lobulated lesions, with fine internal echoes that increased through transmission. (b) T2-weighted MRI shows hyperin-tense lobular lesions in segment 4. (c) T1-weighted MRI demonstrates high signal intensity content within the lesion (asterisks), corresponding to mucoid material.
Table 2.5 Liver calcifications
Diagnosis
Findings
Comments
Metastases after chemotherapy
Neuroblastoma lesions may have calcifications, especially postchemotherapy.
Hepatoblastoma: more evident in mixed type after chemotherapy. Hepatocellular carcinoma: calcifications frequent in fibrolamellar scar. Hemangiomas: calcifications with involution.
Nodular regenerative hyperplasia: calcification is seen in only 1% of patients.
Granulomas
After acute disease, abscesses finally resolve into a calcified granuloma.
In infectious diseases.
Echinococcal cysts
Calcification in cyst wall or complete calcium replacement.
Postinfarct calcifications
After partial hepatic resection or in liver transplant after an ischemic episode (hepatic artery thrombosis or stenosis). The larger areas of infarction may occasionally calcify.
Portal venous system or umbilical veins
In preterm infants.
Calcified hematoma (sequela of biopsy or trauma)
Calcification in the site of biopsy.
Only gold members can continue reading. Log In or Register to continue