, Joungho Han2, Man Pyo Chung3 and Yeon Joo Jeong4
(1)
Department of Radiology Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea, Republic of (South Korea)
(2)
Department of Pathology Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea, Republic of (South Korea)
(3)
Department of Medicine Division of Pulmonary and Critical Care Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea, Republic of (South Korea)
(4)
Department of Radiology, Pusan National University Hospital, Busan, Korea, Republic of (South Korea)
Abstract
Atelectasis is derived from the Greek words ateles and ektasis meaning “incomplete expansion or stretching” [1]. The terms “atelectasis,” “collapse,” and “loss of lung volume” are used synonymously implying reduced inflation of the lung. In broad sense, atelectasis denotes diminished air within the lung associated with volume decrease, and generally, it manifests as increased density. Atelectasis can be differentiated by its volume decrease from consolidation in which volume is maintained because air is replaced by liquid or cells of approximately equal volume (Figs. 11.1, 11.2, 11.3, 11.4, 11.5, 11.6, and 11.7).
Definition
Atelectasis is derived from the Greek words ateles and ektasis meaning “incomplete expansion or stretching” [1]. The terms “atelectasis,” “collapse,” and “loss of lung volume” are used synonymously implying reduced inflation of the lung. In broad sense, atelectasis denotes diminished air within the lung associated with volume decrease, and generally, it manifests as increased density. Atelectasis can be differentiated by its volume decrease from consolidation in which volume is maintained because air is replaced by liquid or cells of approximately equal volume (Figs. 11.1, 11.2, 11.3, 11.4, 11.5, 11.6, and 11.7).





Get Clinical Tree app for offline access
Fig. 11.1
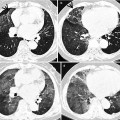
Right upper lobar atelectasis associated central squamous cell carcinoma in a 53-year-old man. (a, b) Lung window images of CT scans (5.0-mm section thickness) obtained at levels of the aortic (a) and azygos (b) arches, respectively, show the atelectatic right upper lobe. Also note the atelectatic right upper lobe marginated posteriorly by the right major fissure (arrowheads) and superiorly elevated right middle lobe marginated by right minor fissure (arrows). RUL right upper lobe, RML right middle lobe, RLL right lower lobe. (c) 18Fluorine fluorodeoxyglucose (FDG) PET demonstrates increased FDG uptake (arrows) within central bronchogenic carcinoma. The atelectatic right upper lobe surrounds the tumor
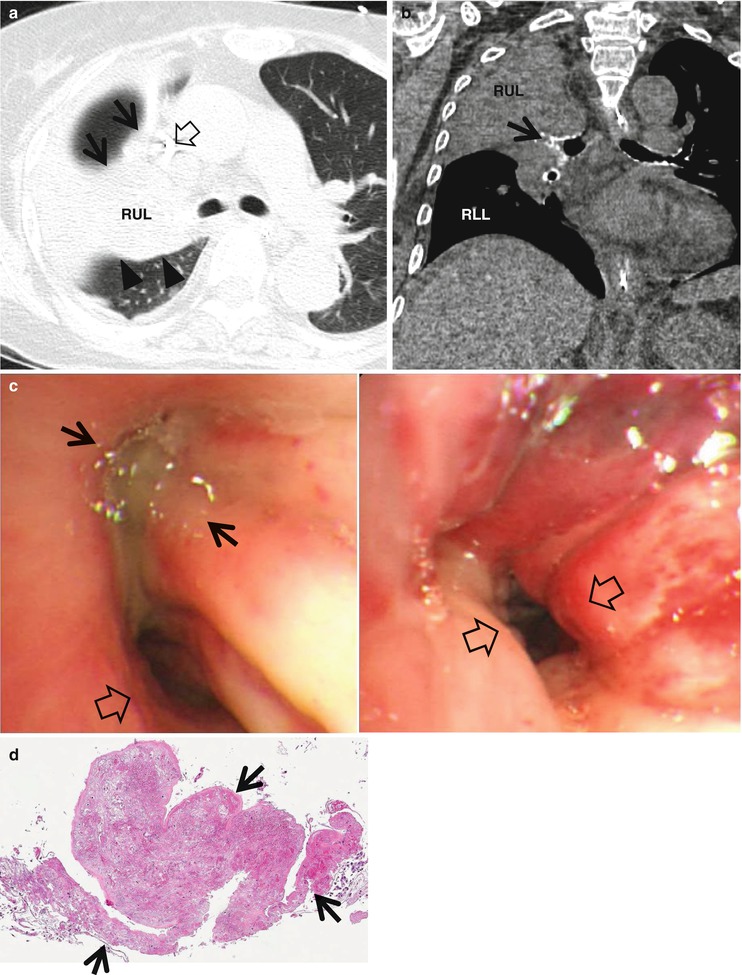
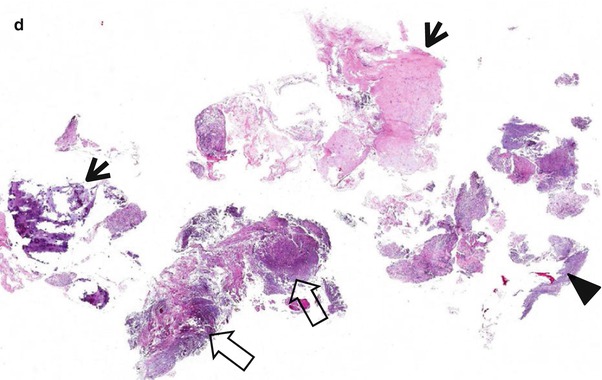
Fig. 11.2
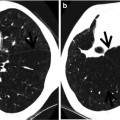
Right upper lobe atelectasis due to bronchial aspergillosis in a 62-year-old woman who has diffuse large B-cell lymphoma. (a) Lung window image of CT scan (2.5-mm section thickness) obtained at level of the main bronchi shows the atelectatic right upper lobe bounded anteriorly by right minor fissure (arrows) and posteriorly by right major fissure (arrowheads). A central venous line (open arrow) is inserted for chemotherapy. RUL right upper lobe. (b) Coronal reformatted image (2.0-mm section thickness) demonstrates the obliterated right upper lobar bronchus (arrow) with intraluminal soft tissue, causing right upper lobar atelectasis. Also note diffuse calcification in airway walls. RUL right upper lobe, RLL right lower lobe. (c) Bronchoscopy displays obliterated the right upper lobar bronchus (arrows) with white necrotic tissue and surrounding mucosal inflammation and edema. The right bronchus intermedius also demonstrates 50 % luminal narrowing (open arrows) with edema and inflammation. (d) High-magnification (×200) photomicrograph of pathologic specimen obtained with bronchoscopic biopsy discloses numerous fungal hyphae (arrows) infiltrating bronchial wall
Fig. 11.3
Left upper lobar atelectasis owing to mucoepidermoid carcinoma arising from the left upper lobar bronchus in a 69-year-old woman. (a) Enhanced CT scan (2.5-mm section thickness) obtained at level of the distal left main bronchus shows an endobronchial nodule (arrow) obstructing the left upper lobar bronchus. Also note the atelectatic left upper lobe (arrowheads). (b) Coronal reformatted (2.0-mm section thickness) CT scan demonstrates endobronchial nodule (arrow) and the atelectatic left upper lobe (arrowheads). (c) Bronchoscopy displays whitish-yellow nodule (arrows) obstructing the left upper lobar bronchus. (d) High-magnification (×100) photomicrograph of pathologic specimen obtained with left upper lobectomy discloses glandular spaces containing mucus (arrows) admixed with sheets of epidermoid cells (open arrows), diagnostic of mucoepidermoid carcinoma
Fig. 11.4
Right middle lobar atelectasis (right middle lobe syndrome) in a 72-year-old man. (a, b) Consecutive CT scans (1.5-mm section thickness) obtained at level of the right inferior pulmonary vein show the atelectatic right middle lobe marginated by right minor (arrows) and major (arrowheads) fissures. Anterior margin (right minor fissure) of the atelectatic right middle lobe is somewhat wavy, whereas posterior margin (right major fissure) of the lobe is sharp
Fig. 11.5
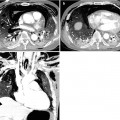
Right lower lobar atelectasis in a 61-year-old man who has squamous cell carcinoma involving the right lower lobe. (a) Mediastinal window image of enhanced CT scan (2.5-mm section thickness) obtained at ventricular level shows low-attenuation mass (arrows) and associated right lower lobar atelectasis (enhancing area, arrowheads). Also note right pleural effusion. (b) 18Fluorine fluorodeoxyglucose (FDG) PET demonstrates increased FDG uptake (arrows) within central bronchogenic carcinoma. The atelectatic right lower lobe surrounds the tumor
Fig. 11.6
Left lower lobar atelectasis related to aspirated foreign body in an 82-year-old woman. (a) Lung window of CT scan (2.5-mm section thickness) obtained at the left lower lobar bronchus level shows the narrowed left lower lobar bronchus (arrow) and volume decrease of left lower lobe bounded laterally by left major fissure (arrowheads). (b




Related posts:

Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
