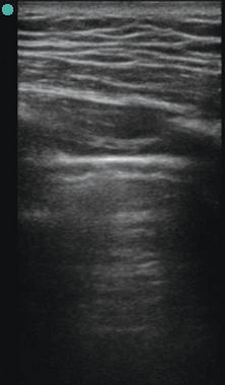
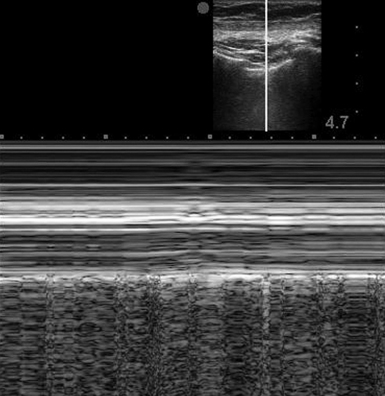
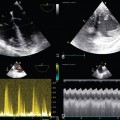
19 Sonographic reverberations of the pleural line. These hyperechoic horizontal lines appear at regular intervals deep to the pleural line and between the rib shadows. Also called a lung rocket, this hyperechoic vertical sonographic artifact arises from the inferior aspect of the pleural line and extends to the edge of the screen without fading. B-lines obscure A-lines and move with lung sliding. Also called the stratosphere sign, this is an M-mode pattern of uninterrupted horizontal lines only, indicative of a lack of normal aeration. A general term for hyperechoic vertical sonographic artifacts that may be present during lung ultrasound. B-lines are a type of comet tail. Dynamic and static air bronchogram: Sonographic air bronchograms are tubular bright artifactual structures within a tissue, such as lung consolidation; they correspond to air bronchograms on radiographs. On M-mode, static bronchograms will produce straight lines, whereas dynamic bronchograms produce a sinusoidal pattern. A term applied when the lung’s appearance on lung ultrasound resembles that of the liver. A dynamic sign, this is the cyclic appearance of findings associated with aerated lung (lung sliding, A- or B- lines) creeping into and then out of view with each respiratory cycle. Similar to lung sliding, this dynamic sign is perceived as shimmering of the pleural line in concert with the heartbeat and is commonly seen at the left anterior chest wall. A dynamic sign perceived as shimmering of the pleural line in association with respiration. This sign is an M-mode pattern of uninterrupted horizontal lines superficial to the pleural surface with a granular pattern deep to this level; it indicates a normal aeration pattern in an inflating and deflating lung. See barcode sign. General chest ultrasound (lung ultrasound and echocardiography) is a core element of the holistic approach to critical care ultrasound presented in Chapter 1. Lung ultrasound and echocardiography are illustrated in Chapters 19 to 24 and Chapters 26 to 34, respectively; moreover, features of hemodynamic monitoring in the intensive care unit (ICU) are presented in Chapters 36 to 40. A low-frequency transducer, 3.5 to 5.0 MHz, is positioned in longitudinal orientation over the chest wall in an intercostal space with the probe marker held cranially by convention. Gain and depth settings are adjusted to focus attention at the space between the rib shadows. The pleural line (Figure 19-1), a bright hyperechoic horizontal linear structure, is visualized between the rib shadows. A dynamic sign perceived as shimmering of the parietal and visceral pleura in contact is referred to as lung sliding and is part of the normal aeration pattern. Confirmation of lung sliding can be pursued with the use of M-mode. Directing the ultrasound beam between the rib shadows to transect the pleural line allows analysis of motion over time in the single-dimensional interface at that location. In the presence of normal pleural interaction, the resulting screen after initiating M-mode will display a pattern referred to as the seashore sign (Figure 19-2). Horizontal lines superficial to the pleural surface indicate a lack of motion of the chest wall structures with respiration. Deep to this is a bright hyperechoic horizontal line (representing the pleural surface), and immediately deep to the pleural line is a granular pattern indicating a normal aeration pattern in an inflating and deflating lung. Evaluation of the lung parenchyma is based on the presence of different artifact patterns, all of which emanate from the pleural line. The A-line (Figure 19-3) is a reverberation of the pleural line, and given an adequate depth setting, several of these parallel lines can be seen at regular intervals. When visualized in the presence of lung sliding, an A-line–dominant pattern is said to occur and is suggestive of normal lung parenchyma. In addition, an A-line–dominant pattern is noted to correlate with low pulmonary capillary wedge pressure and hence represents a low likelihood for pulmonary edema.1
Lung ultrasound: The basics
The normal lung
Evaluation for pneumothorax
Related posts:
 Ultrasound-guided peripheral intravenous access
Ultrasound-guided peripheral intravenous access
 Ultrasound-guided arterial catheterization
Ultrasound-guided arterial catheterization
 Ultrasound-guided placement of inferior vena cava filters: (CONSULTANT-LEVEL EXAMINATION)
Ultrasound-guided placement of inferior vena cava filters: (CONSULTANT-LEVEL EXAMINATION)
 Ultrasonography in circulatory failure
Ultrasonography in circulatory failure
 Evaluation of right ventricular function in the intensive care unit by echocardiography: (CONSULTANT-LEVEL EXAMINATION)
Evaluation of right ventricular function in the intensive care unit by echocardiography: (CONSULTANT-LEVEL EXAMINATION)
 Procedural ultrasound for surgeons: (CONSULTANT-LEVEL EXAMINATION)
Procedural ultrasound for surgeons: (CONSULTANT-LEVEL EXAMINATION)
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Radiology Key
Fastest Radiology Insight Engine