18
Lymphoma
Eugene C. Lin and Abass Alavi
Positron emission tomography (PET) is a standard modality for staging both Hodgkin disease (HD) and non-Hodgkin lymphoma (NHL) (Figs. 18.1, 18.2, and 18.3).
- Hodgkin disease. In HD, PET can be of value in any stage, but it is most useful in stage I and II disease, where a change in stage will alter disease management. Overall, PET changes management in a median of 14% of patients.2
- NHL. In NHL, PET can be of value in any stage, but it is most useful in staging aggressive disease. It is very helpful as a baseline test if PET is to be used to monitor response to treatment.
- Stage. PET may be more useful in stage I disease (some centers use the same therapy for all stages of aggressive NHL except stage I).
- Histology. PET may have a role in the staging of low-grade follicular NHL. PET is of questionable value in other sub types of low-grade NHL, such as small lymphocytic and mucosa-associated lymphoid-type (MALT) lymphoma.3 PET may be of potential value in mantle cell lymphoma.
- PET. Sensitivity 90%, specificity 91%4
- HD. Sensitivity 93%, specificity 88%
- NHL. Sensitivity 87%, specificity 94%
Fig. 18.1 Extensive lymphoma. Coronal positron emission tomography scan in a patient with non-Hodgkin lymphoma demonstrates uptake in mediastinal, supraclavicular, axillary, and retroperitoneal nodes, liver, and bone marrow (pelvis and lumbar spine).
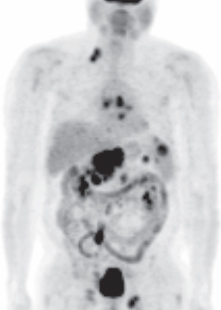
Fig. 18.2 Extensive lymphoma. Coronal positron emission tomography scan in a patient with non-Hodgkin lymphoma demonstrates uptake in mediastinal, supraclavicular, abdominal, pelvic, and groin nodes and the spleen.
- PET/computed tomography (CT). Improved staging accuracy by 9%5
- Histological subtype. PET has variable sensitivity depending on the histological subtype of lymphoma.6 In general, PET has high sensitivity in the three major classes of this malignancy in clinical practice–diffuse large B cell and follicular lymphomas and Hodgkin disease.
- Hodgkin disease. The different histological subtypes of Hodgkin disease all have substantial FDG uptake, although the difference in degree of uptake is significant among the subtypes. Mixed cellularity has the most uptake, followed by nodular sclerosis and nodular lymphocytic predominant type.7 However, the fluorodeoxyglucose (FDG) uptake in the least FDG-avid subtype (lymphocytic predominance) is very high.
- Non-Hodgkin lymphoma. The sensitivity of PET in low-grade NHL depends on histology. Sensitivity is excellent in follicular lymphoma, moderate in marginal zone lymphoma, and poor in small celllymphocytic lymphoma.8 The higher grade lymphomas are in general more FDG avid, but sensitivity in peripheral T cell lymphoma is moderate.6 Patients with NHL and standardized uptake value (SUV) > 10 have a high likelihood of aggressive disease.9
- Follicular lymphoma. PET is accurate in both indolent and aggressive nodal follicular lymphoma.10 Low-grade follicular lymphomas of the gastrointestinal tract usually have substantial FDG uptake,11 but the degree of uptake is still less than that in high-grade NHL. However, sensitivity for bone marrow involvement in follicular lymphoma is limited.12
- Marginal zone lymphoma (MZL). PET has good sensitivity for nodal MZL but has poor sensitivity for extranodal MZL (in particular, splenic MZL). 13,14
- Mucosa-associated lymphoid tissue lymphoma. PET has variable sensitivity for MALT lymphoma. The sensitivity in patients with advanced disease is much higher than that in early-stage disease.15 The sensitivity of PET in typical MALT lymphomas is low, but MALT lymphomas with plasmacytic features usually have substantial FDG uptake.16 MALT lymphomas of the gastrointestinal tract typically have low FDG uptake.11
- Peripheral T cell lymphoma. PET has high sensitivity at nodal and noncutaneous nodal sites but poor sensitivity at cutaneous sites17 and for bone marrow involvement.18 FDG uptake in cutaneous T cell lymphoma is much more likely in stage IV disease.2
- Anatomical region. PET is more sensitive in the thorax than the abdomen/pelvis.19
- Bone marrow involvement. PET is able to detect sites of bone marrow involvement not sampled with iliac crest biopsy. Initial studies suggested that PET is more sensitive and specific than bone scintigraphy or CT for bone marrow involvement. However, later studies suggest a lower sensitivity for bone marrow involvement, particularly in low-grade NHL.6 In particular, although PET has good sensitivity in nodal follicular lymphoma,10 the sensitivity for bone marrow involvement is limited.12 The overall sensitivity and specificity of PET for bone marrow involvement (compared with bone marrow biopsy) are 51% and 95%, respectively.20 The sensitivity is higher in HD and high-grade NHL.
- Splenic disease. PET is 97% accurate for the diagnosis of splenic involvement in HD.
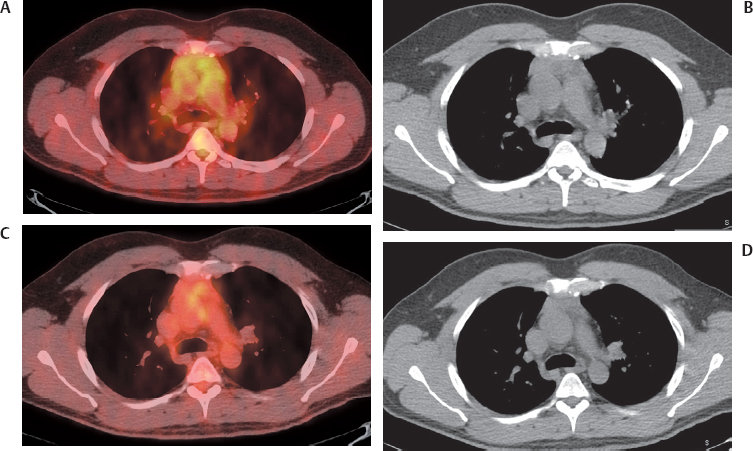
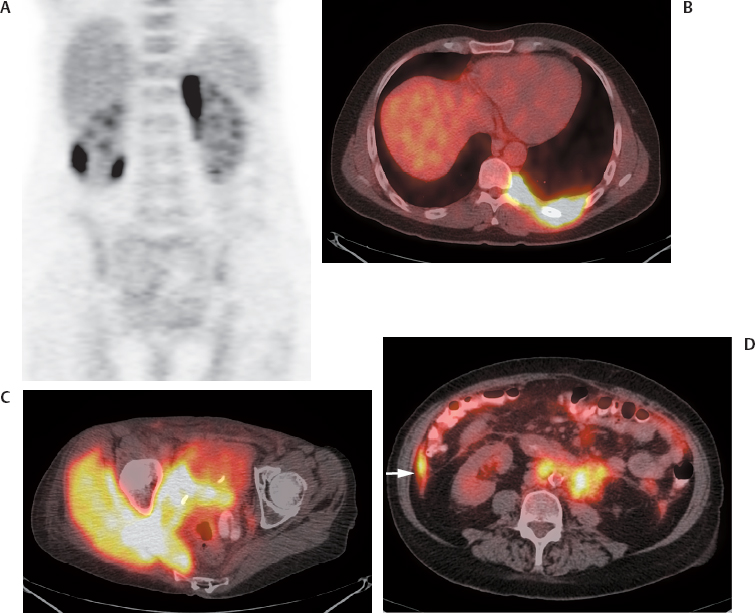
Fig. 18.3 Lymphoma: spectrum of disease. Positron emission tomography (PET) and PET/computed tomography scans in different patients with non-Hodgkin lymphoma demonstrate disease involving the (A) perirenal space, (B) pleura, (C) muscle, and (D) peritoneum (arrow).
- This was generated by using a degree of uptake greater than that of the liver as evidence of splenic disease.21
- PET is particularly more accurate for detecting focal splenic involvement than gallium or CT.
Comparison with Other Modalities
- PET versus CT. PET and CT have comparable specificity, but PET is ~15% more sensitive.19
- The primary advantage of PET over CT is in nodal detection in the thorax and periphery; in the abdomen and pelvis, PET and CT provide comparable results.22,23
- PET and CT are concordant in staging 80 to 90% of patients with diffuse large B cell and follicular lymphoma. In contrast, PET and CT are less likely to be concordant in staging HD (60 to 80%).24 In both cases, PET discordance usually results in upstaging. However, the higher rate of discordance in HD suggests that both PET and CT need to be performed in staging HD.
- PET/CT versus CT. PET/CT (with low-dose nonenhanced CT) is more sensitive and specific than contrast-enhanced CT for both nodal and extranodal disease.
- PET/CT is particularly valuable compared with CT in the exclusion of disease.
- A common problem with CT is false-positive results from lung opacities interpreted as lymphoma; these can be accurately diagnosed by PET.
- Nodal disease (Table 18.1)
- Extranodal disease (Table 18.2)
- PET versus gallium. PET is superior to gallium for both initial staging and follow-up of lymphoma.25
- Thymus. It is important to recognize thymic hyperplasia as a distinct entity in patients with anterior mediastinal uptake. Thymic hyperplasia (as seen in Figs. 6.19, p. 52 and 6.20, p. 53) is a common reaction following chemotherapy and as such is an expected phenomenon.
- Diffuse bone marrow activity. Bone marrow uptake postgranulocyte colony-stimulating factor (G-CSF) therapy (as seen in Fig. 6.30, p. 58) can mimic or obscure lymphomatous bone marrow infiltration.
- Focal bone marrow activity. Always consider a history of prior bone marrow biopsy as a cause of focal uptake in the posterior ilium.
- Spleen
- Splenic uptake post G-CSF therapy can mimic splenic involvement (as seen in Fig. 6.30, p. 58).
- The spleen is a common site for false-positive findings from infectious/inflammatory etiologies.
- Low-grade lymphomas. Certain low-grade lymphomas, such as small-cell lymphocytic lymphoma, typically do not have substantial FDG uptake and may not be detected with high sensitivity by PET. In these cases, a positive scan often demonstrates hazy mild uptake.
- PET is increasingly employed as a standard modality for assessing response to therapy in both HD and aggressive NHL (Fig. 18.4). It is particularly useful in later stages of the disease, when response to chemotherapy is substantially lower than that in early stages.
 Staging
Staging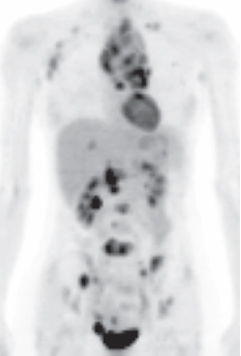
 Therapy Response26–28
Therapy Response26–28