Anterior knee pain is associated with many different causes. The clinical diagnosis may be unclear when the patient initially presents for evaluation. Magnetic resonance (MR) imaging is a valuable modality with high diagnostic accuracy in the evaluation of extensor mechanism pathology, which commonly presents with anterior knee pain. The most common disorders include patellar fracture, patellofemoral tracking abnormalities, tendon trauma and degeneration. These injuries manifest with characteristic patterns on MR imaging. This article discusses normal anatomy, common injuries, and diagnostic pitfalls on MR imaging.
Key points
- •
Magnetic resonance (MR) imaging shows high diagnostic accuracy in the characterization of extensor mechanism disorders, especially when the clinical diagnosis is unclear.
- •
Knowledge of characteristic patterns of injury on MR imaging increases detection of injury.
- •
Radiologists must be aware of common anatomic variants and imaging pitfalls of the extensor mechanism as seen on MR imaging.
Introduction
Anterior knee pain, a common clinical complaint, is one of the most frequent referrals for magnetic resonance (MR) imaging of the lower extremity. Types of quadriceps and patellar tendon injury include acute traumatic rupture, chronic repetitive/overuse injury, and tendon degeneration. Patellofemoral instability, patellar dislocation, and tracking abnormalities are common disorders.
Although radiography is the first-line imaging modality in the acute traumatic setting, and ultrasonography is used in the diagnosis of soft tissue injury, MR imaging shows high diagnostic accuracy in the evaluation of anterior knee pain when the physical examination is limited, when the clinical presentation is unclear, or when injury that is occult on radiography is suspected. MR imaging is particularly well suited to imaging the soft tissues because of its high soft tissue contrast and resolution. However, it is important to be aware of common MR imaging pitfalls when evaluating disorders of the extensor mechanism.
Introduction
Anterior knee pain, a common clinical complaint, is one of the most frequent referrals for magnetic resonance (MR) imaging of the lower extremity. Types of quadriceps and patellar tendon injury include acute traumatic rupture, chronic repetitive/overuse injury, and tendon degeneration. Patellofemoral instability, patellar dislocation, and tracking abnormalities are common disorders.
Although radiography is the first-line imaging modality in the acute traumatic setting, and ultrasonography is used in the diagnosis of soft tissue injury, MR imaging shows high diagnostic accuracy in the evaluation of anterior knee pain when the physical examination is limited, when the clinical presentation is unclear, or when injury that is occult on radiography is suspected. MR imaging is particularly well suited to imaging the soft tissues because of its high soft tissue contrast and resolution. However, it is important to be aware of common MR imaging pitfalls when evaluating disorders of the extensor mechanism.
Normal anatomy
The extensor mechanism is composed of the quadriceps femoris tendon and muscles, the patella and patellofemoral joint, and the patellar tendon. The quadriceps tendon is a trilaminar structure formed by the coalescence of the 4 quadriceps tendons, inserting on the superior pole of the patella. The rectus femoris forms the most anterior layer of the quadriceps tendon. The vastus medialis and lateralis together form the intermediate layer, and the vastus intermedius forms the deepest layer. There is ongoing debate in the literature as to the anatomy of the vastus medialis muscle. Two sets of muscle fibers have been described: the vastus medialis longus proximally, and the vastus medialis obliquus, which extends distally to insert on the medial patella. There is no consensus in the literature as to whether these two components are separate muscles, or whether they reflect different directional fibers of the same muscle. On MR imaging, the normal appearance of the trilaminar quadriceps tendon manifests as low-signal tendon fibers with interdigitating fat ( Fig. 1 ).
The patella is the largest sesamoid in the body and lies between the quadriceps and patellar tendons. Superficial quadriceps fibers extend over the patella to insert on the tibial tuberosity as part of the patellar tendon, termed the prepatellar quadriceps continuation. The patella plays an important role in extensor mechanism function. The patella protects the distal femoral articular cartilage, links the quadriceps and patellar tendons, and provides increased mechanical leverage of the quadriceps muscles during extension by elevating the extensor tendons from the axis of rotation of the knee, increasing the angle over which the quadriceps tendon can act.
The patella has a large, shallow lateral facet and a steeper, shorter medial facet separated by a vertically oriented median ridge. Many patellae also show a medially located odd facet in the medial facet ( Fig. 2 ). When the knee is in extension, the patella articulates with the shallow portion of the proximal femoral trochlea; it is in this position that the patella is most prone to subluxation or dislocation. When the knee is flexed, the patella is fully engaged within the femoral trochlea. The normal patella shows marrow and cortical signal on all pulse sequences.
The patella is stabilized by the medial and lateral patellar retinacula. The medial patellar retinaculum has been variously described as having 2 or 3 layers; these layers can be difficult to distinguish on MR imaging in normal patients. The most important medial patellar stabilizer is the medial patellofemoral ligament (MPFL), which extends from the medial patella to the medial epicondyle of the distal femur. The lateral retinaculum stabilizes the lateral patella. The normal retinacula show low signal on all pulse sequences ( Fig. 3 ).
The patellar tendon is a thick, bandlike structure that extends from the inferior pole of the patella and fans out to insert on the anterior tibial tubercle. The normal patellar tendon is oriented along the axis of the proximal tibia. The normal patellar tendon shows homogeneous low signal intensity on all pulse sequences with the exception of normal, mildly increased signal at the posterior margins of the origin and insertion sites of the tendon.
The quadriceps fat pad lies deep to the quadriceps tendon insertion on the patella, and anterior to the suprapatellar recess. The normal quadriceps fat pad is triangular in shape and demonstrates fat signal on all pulse sequences. The extrasynovial, intracapsular, infrapatellar fat pad (IPFP), or fat pad of Hoffa, lies between the patellar tendon and the anterior knee joint. It is thought that the IPFP may serve to facilitate knee function, increase lubrication of the joint, and may even play a role in inflammation and degeneration of the knee joint. The normal IPFP shows fat signal.
Three bursae are present within the anterior knee. The prepatellar bursa lies in the subcutaneous tissues superficial to the patella. The superficial infrapatellar bursa lies anterior to the patellar tendon insertion on the tibia, and the deep infrapatellar bursa lies between the distal patellar tendon and its insertion on the anterior tibial tubercle.
The suprapatellar recess extends cranially from the knee joint, posterior to the quadriceps fat pad and anterior to the prefemoral fat pad. The suprapatellar recess extends medially and laterally over the medial and lateral femoral condyles, and communicates with the medial and lateral recesses beneath each retinaculum. The suprapatellar recess and the joint capsule are stabilized while in extension by the articular muscle of the knee, also known as the musculus articularis genus. This muscle originates from the distal femur and can be seen in most patients on sagittal MR imaging ( Fig. 4 ).
The extensor mechanism does not have a paratenon. The genicular arteries provide blood supply to the patella and secondarily to the quadriceps and patellar tendons. The relative avascularity of the quadriceps and patellar tendons at their osseous insertions may explain why the quadriceps and patellar tendons tear so frequently in this location. The extensor mechanism is supplied additionally by the IPFP, anterior subcutaneous tissues, and the joint capsule.
Quadriceps injury
Quadriceps Rupture and Partial Tear
Acute quadriceps rupture occurs in the setting of sports injury or in the context of chronic quadriceps degeneration or previous trauma. Rupture occurs most frequently in men more than 40 years of age, and is also associated with underlying systemic disease or medications, such as renal failure, diabetes, gout, hyperparathyroidism, rheumatoid arthritis, systemic lupus erythematosus, obesity, and steroid and fluoroquinolone use. Bilateral spontaneous ruptures have been reported in patients with gout, diabetes, and steroid use. Ruptures occur most frequently at the insertion of the quadriceps on the patella. Complete quadriceps ruptures are much less common than partial quadriceps tears. MR imaging has been shown to be of higher specificity than ultrasonography for determining whether the quadriceps tear is complete or partial, and thus MR imaging is important for presurgical planning.
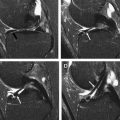
MR imaging findings of complete quadriceps rupture show fluid signal within a torn and retracted quadriceps tendon; no fibers are identified inserting on the patella. The quadriceps stump retracts cranially and the patella retracts caudally, often associated with a wavy appearance of the patellar tendon. There is frequently a large joint effusion with hematoma at the rupture site ( Fig. 5 ). Avulsion fragments may be identified at the quadriceps stump. MR imaging of partial quadriceps tear shows discontinuity of any of the layers of the quadriceps tendon but without complete tendon disruption ( Fig. 6 ). The anteriormost rectus femoris is most frequently torn. Injury may also involve the prepatellar quadriceps continuation, which should not be mistaken for prepatellar bursitis ( Fig. 7 ).
It is important to differentiate between complete quadriceps ruptures and partial tears, because the treatments are substantially different. Acute quadriceps full-thickness rupture is treated surgically by tunneling the quadriceps tendon into the patella. If the rupture is chronic, or occurs in the setting of a total knee arthroplasty, then the repair may require a tendon graft. If the tear is partial, treatment is conservative.
Quadriceps Tendinosis
Tendinosis of the quadriceps is less common than patellar tendinosis, and occurs most frequently in the setting of chronic underlying systemic disease and/or drug use, as discussed earlier. Calcific tendinosis of the quadriceps tendon has been described. In addition, repetitive microtrauma such as that seen in jumping sports is associated with tendinosis. MR findings show a thickened, abnormal tendon with increased intermediate signal in the tendon fibers ( Fig. 8 ).
Patellar tendon injury
Overuse Injuries
Patellar tendinosis is the most commonly encountered disorder of the patellar tendon. Also known as jumper’s knee, it typically is seen in a young active population and is commonly associated with running and jumping. This diagnosis can be confirmed with MR imaging, with sagittal and axial fluid-sensitive sequences being the most useful; thickening and increased signal of the tendon proximally at its attachment to the inferior patellar pole are the most common findings in acute cases ( Fig. 9 ). Bone marrow edema in the inferior patellar pole can also be seen in severe cases. Chronic cases of patellar tendinosis may show thickening and abnormal signal involving the entire tendon with abnormal signal intensity on both T1-weighted and T2-weighted sequences. Other described chronic imaging findings include periosteal reaction along the anterior margin of the patella, calcification within the patellar tendon, and elongation of the inferior patellar pole.
Osgood-Schlatter Disease
Repetitive stress or overuse injuries of the patellar tendon such as Osgood-Schlatter disease is caused by chronic traction of the patellar tendon at the level of the tibial tubercle. The apophyseal cartilage of the tibial tuberosity is weak compared with the tensile forces of the extensor mechanism, resulting in fragmentation of the bone and cartilage. This diagnosis is often made clinically with additional imaging usually obtained to exclude other causes of anterior knee pain. When MR imaging is obtained, typical findings include fragmentation and edema of the tibial tubercle with surrounding soft tissue edema. The patellar tendon is also thickened with increased signal distally at the level of the tibial tubercle on the fluid-sensitive sequences ( Fig. 10 ). Irregularity of the tibial tubercle often persists into adulthood even when no longer symptomatic.
Sinding-Larsen-Johansson Syndrome
Sinding-Larsen-Johansson syndrome is overuse injury of the proximal patellar tendon at the level of the inferior patellar pole. The inferior patellar pole can appear fragmented and show abnormal hyperintense signal changes on the fluid-sensitive MR sequences depending on the degree of stress injury ( Fig. 11 ). MR imaging is also useful in distinguishing this overuse injury from patellar sleeve fractures.
Patellar Sleeve Fracture
Patellar sleeve fractures are fractures of the inferior pole of the patella with involvement of the unossified patellar cartilage ( Fig. 12 ). MR imaging is important to show the full extent of unossified patellar cartilage involvement, which is significantly underestimated on radiography. Acute tensile forces on the extensor mechanism can also lead to avulsion fractures of the distal patellar tendon ( Fig. 13 ).
Patellar Tendon Tear
Overuse injuries can progress to focal tears of the patellar tendon. Tearing can also occur in the acute setting. Fluid-sensitive MR sequences show focal cleftlike high-intensity signal within the tendon ( Fig. 14 ). Ruptures of the patellar tendon occur but are uncommon. When encountered, patients typically have concomitant systemic disease that predisposes them to such an injury. Patellar tendon ruptures have also been described in certain athletes who receive a substantial direct impact to their anterior knee, such as football players. With MR imaging, there is discontinuity of the patellar tendon with acute tears showing extensive edema of the surrounding soft tissues ( Fig. 15 ). Acute patellar tendon ruptures are managed surgically with transpatellar bone tunnels formed when the rupture occurs at the level of the inferior patellar pole.
Related posts:
 MR Imaging of the Knee
MR Imaging of the Knee
 Magnetic Resonance Imaging of the Meniscus
Magnetic Resonance Imaging of the Meniscus
 Magnetic Resonance Imaging of the Postoperative Meniscus
Magnetic Resonance Imaging of the Postoperative Meniscus
 MR Imaging Assessment of Arthritis of the Knee
MR Imaging Assessment of Arthritis of the Knee
 Quantitative Magnetic Resonance Imaging of the Articular Cartilage of the Knee Joint
Quantitative Magnetic Resonance Imaging of the Articular Cartilage of the Knee Joint
 MR Imaging of Extrasynovial Inflammation and Impingement About the Knee
MR Imaging of Extrasynovial Inflammation and Impingement About the Knee
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


