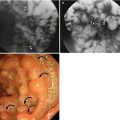
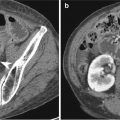
Fig. 22.1
Atypical lipomatous tumor/well-differentiated lipoma (ALT/WDL). (a) On axial contrast-enhanced CT, a large fatty mass is noted around the left kidney. (b, c) Within the fatty mass, irregular septa (arrows) are noted. The fat component appears as high signal intensity and internal septum appears as iso- to low-signal intensity compared to muscle on T1- (b) and T2-weighted images (c). (d, e) Compared to the precontrast T1-weighted fat-saturated image (d), the internal septum shows enhancement after contrast media administration (e). The patient underwent mass excision with radical left nephrectomy and left adrenalectomy (f). On a photograph of the gross specimen, the mass shows multi-lobulated and rubbery texture with mainly bright yellow colors with focal white areas. There was no evidence of necrosis or hemorrhage. The final diagnosis was ALT/WDL
22.7.2 Atypical Lipomatous Tumor/Well-Differentiated Lipoma (ALT/WDL) with Sclerosing Component
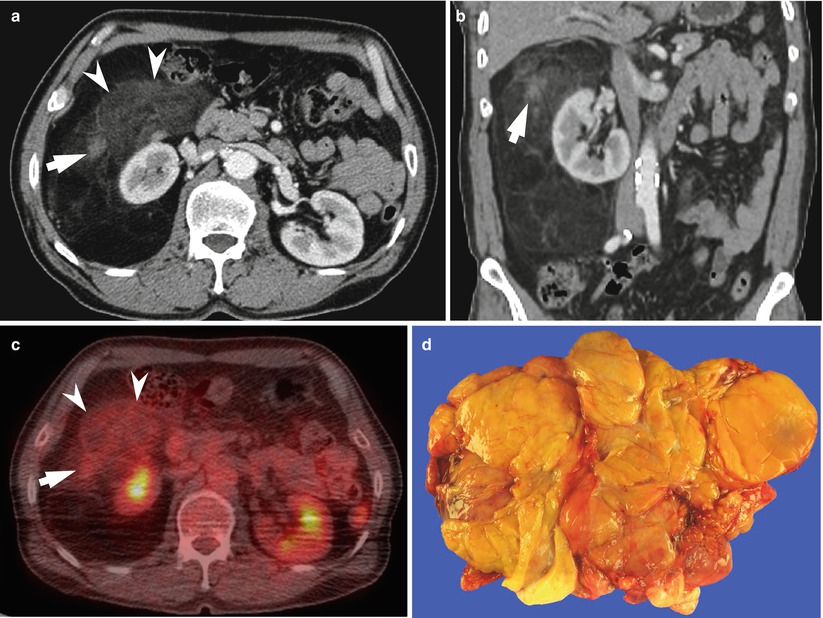
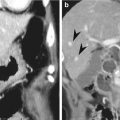
Fig. 22.2
Atypical lipomatous tumor/well-differentiated lipoma (ALT/WDL) with the sclerosing component. (a, b) On axial (a) and coronal (b) contrast-enhanced CT images, a large fatty mass with a small solid component (arrow) and areas of increased attenuation (arrowheads) are noted around the right kidney. The attenuation of the solid component appears similar to that of muscle. (c) On the PET/CT scan, the F-18 FDG uptake increased at the solid component and at areas of increased attenuation. (d) On a photograph of the gross specimen, the lesion appears as a well-circumscribed multi-lobulated mass with separation by whitish fibrous septa. This mass was confirmed as ALT/WDL with the sclerosing component
22.7.3 Dedifferentiated Liposarcoma
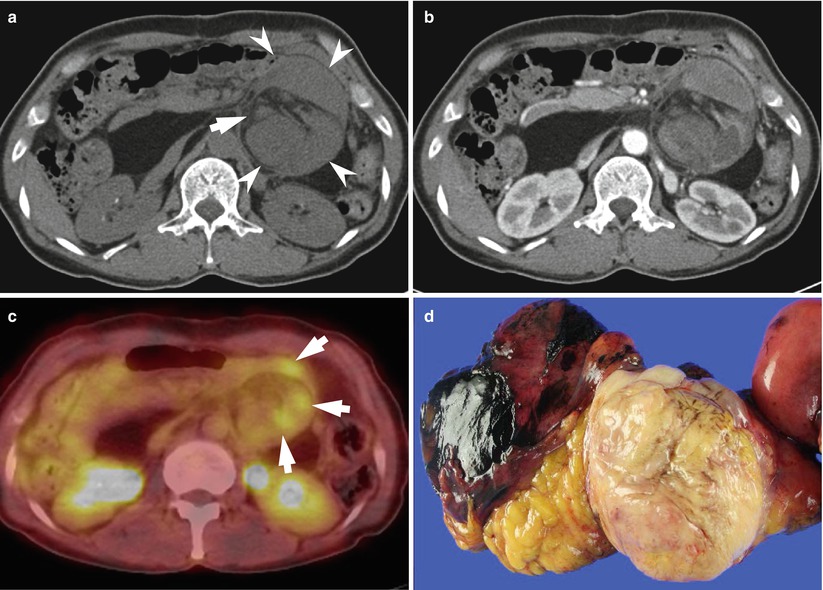
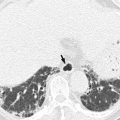
Fig. 22.3
Dedifferentiated liposarcoma. (a) On non-contrast CT, a well-circumscribed mass with fatty (arrow) and non-fatty components (arrowheads) is noted in the left mid abdomen. (b) After contrast enhancement, the non-fatty component shows homogeneous or inhomogeneous enhancement. (c) On PET/CT, the focal increased uptake of F-18 FDG is seen in the non-fatty component (arrows). (d) On a photograph of the gross specimen, a lobulated mass with fatty component and hemorrhage is seen. This lesion was confirmed as dedifferentiated liposarcoma
22.7.4 Dedifferentiated Liposarcoma with Calcification
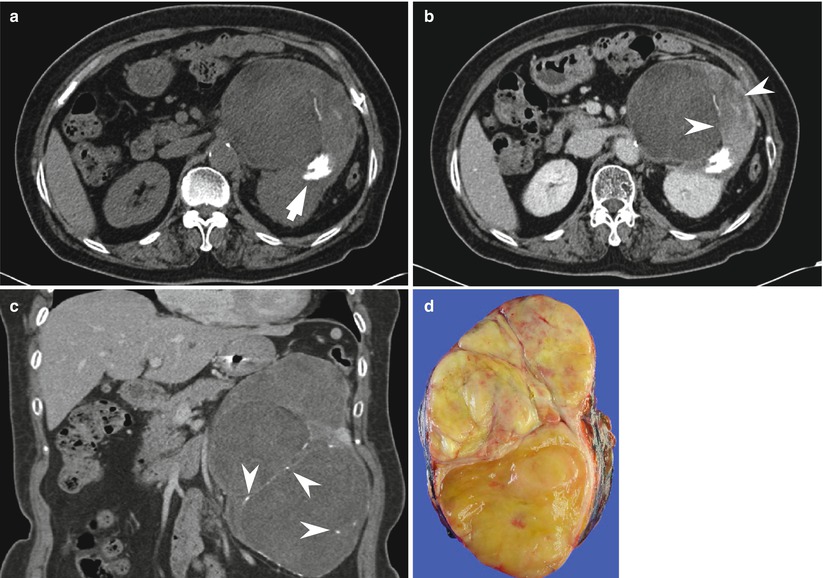
Fig. 22.4
Dedifferentiated liposarcoma with calcification. (a) On non-contrast CT, a well-circumscribed fatty mass with the solid component and dense calcification (arrow) is seen in the left upper abdomen. (b) On contrast-enhanced axial CT image, heterogeneous enhancement is seen in the solid component (arrowheads). (c) On contrast-enhanced coronal CT image, focal or linear calcification is noted in the internal septa of the mass (arrowheads). Mass excision with distal pancreatectomy and splenectomy was performed. (d) On a photograph of the gross specimen, the cut surface shows a pale yellow-colored area with multifocal hemorrhage and fibrous septa. This lesion was confirmed as dedifferentiated liposarcoma
22.7.5 Dedifferentiated Liposarcoma Without Gross Fat Component
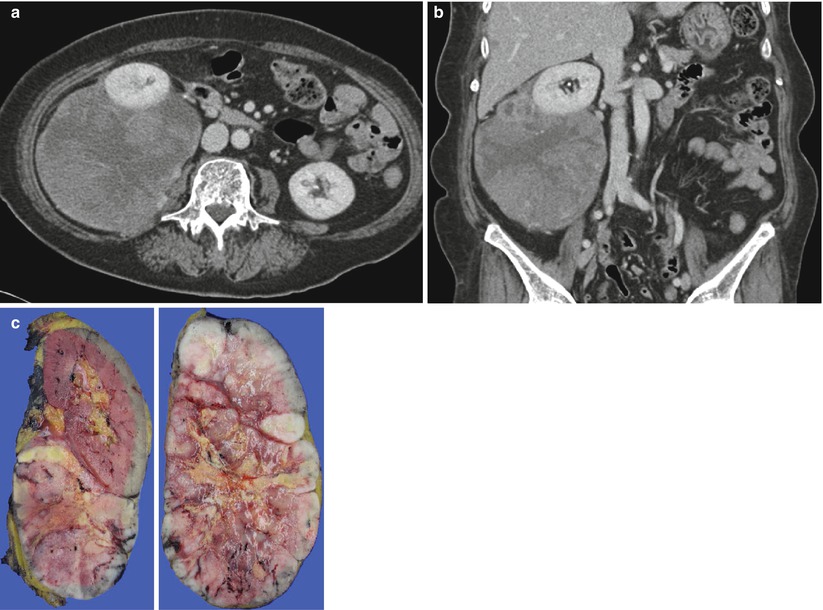
Fig. 22.5
Dedifferentiated liposarcoma without the gross fat component. (a, b) On contrast-enhanced axial (a) and coronal (b) CT images, a well-circumscribed enhancing mass with a central poorly enhancing area is seen at the posteroinferior aspect of right kidney. Mass excision with right nephrectomy was performed. (c) On a photograph of the gross specimen, the cut surface of the mass appears as multi-lobulated whitish tissue with a central yellowish ischemic area and focal hemorrhage. The mass was confirmed as differentiated liposarcoma and the cellular type of dedifferentiation was pleomorphic
22.7.6 Myxoid Liposarcoma
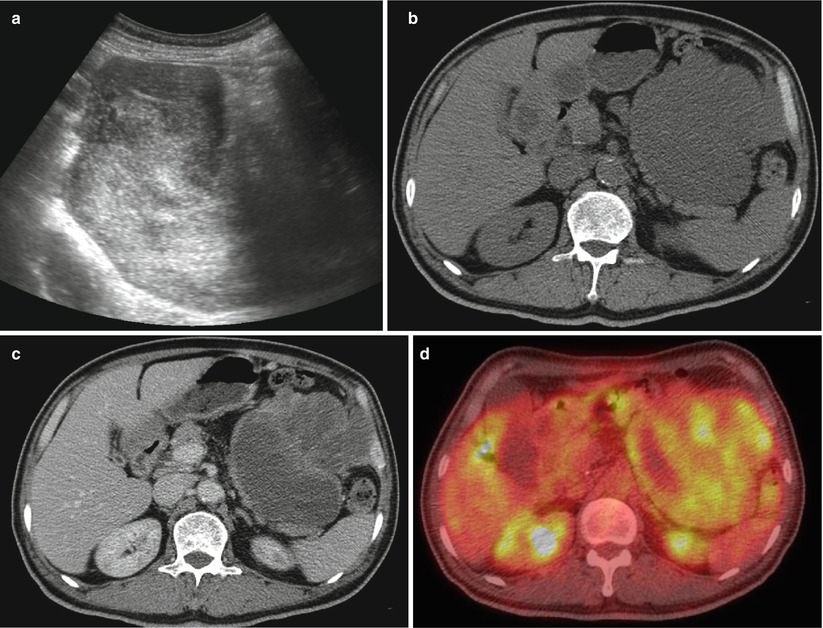
Fig. 22.6
Myxoid liposarcoma. (a) On US, a lobulated, large, heterogeneous, highly echogenic mass is noted in the left upper abdomen. (b) On the non-contrast CT image, the mass manifests as low attenuation similar to cystic lesions. There is no evidence of fat components within the lesion. (c) On the contrast-enhanced CT image, the mass shows heterogeneous enhancement. (d) On PET/CT, an increased uptake of F-18 FDG is seen in the mass. Mass excision was performed and pathology confirmed a diagnosis of myxoid liposarcoma
22.7.7 Myxoid Liposarcoma in the Scrotum
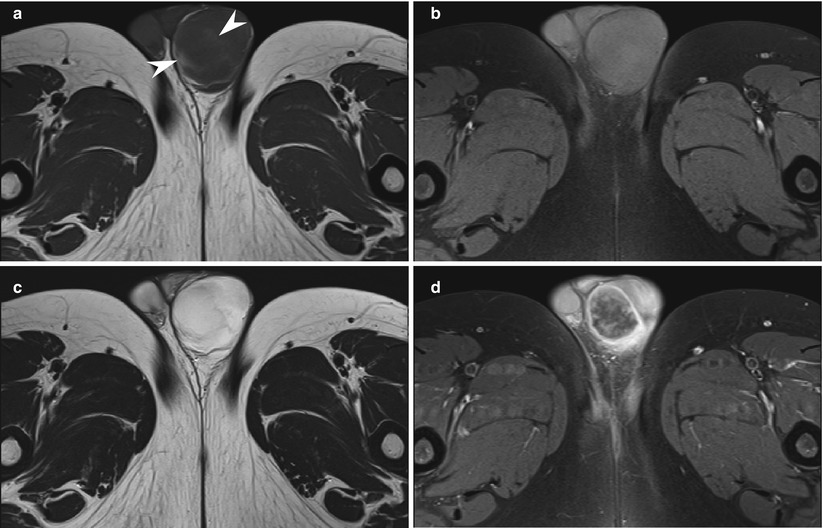
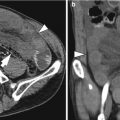
Fig. 22.7
Myxoid liposarcoma in the scrotum. (a, b) On T1-weighted (a) and T1-weighted fat-saturated (b) MR images, a well-circumscribed low SI mass is seen in the left scrotum. An amorphous high SI lesion is noted within the mass (arrowheads in a) before fat saturation. (c) On the T2-weighted MR image, the mass appears as high SI. (d) On the contrast-enhanced T1-weighted image, the peripheral portion of the mass shows well enhancement, whereas the central area only shows patchy enhancement. The mass was excised and the final pathologic diagnosis was myxoid liposarcoma
22.7.8 Pleomorphic Liposarcoma
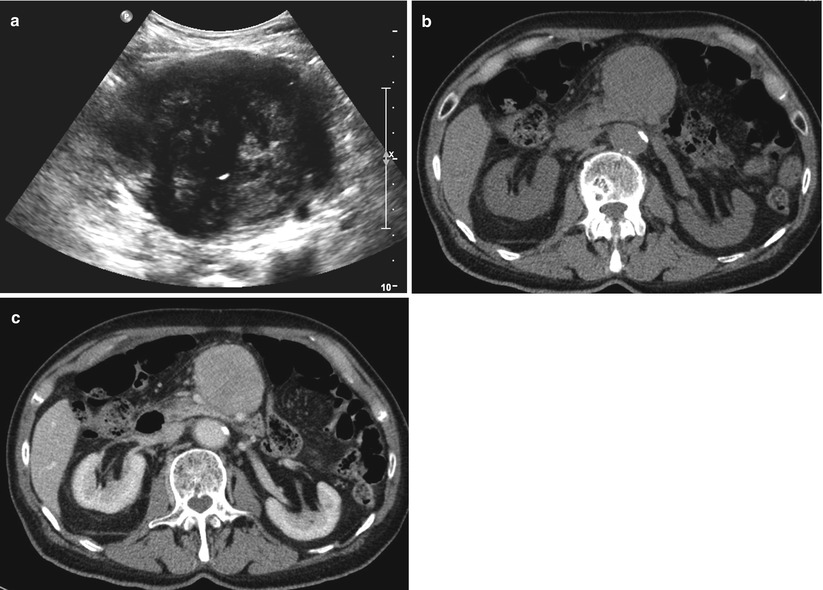
Fig. 22.8
Pleomorphic liposarcoma. (a) On US, a well-circumscribed round mass with heterogeneous echogenicity is noted in the mid abdomen. (b) On the non-contrast CT image, a round homogeneous low attenuating mass is seen at the mesentery. The attenuation of mass was similar to that of the muscle or liver parenchyma. (c) After contrast enhancement, the mass showed homogeneous enhancement. Mass excision was performed and pathology confirmed a diagnosis of pleomorphic liposarcoma
22.7.9 Solitary Fibrous Tumor in the Pelvic Cavity
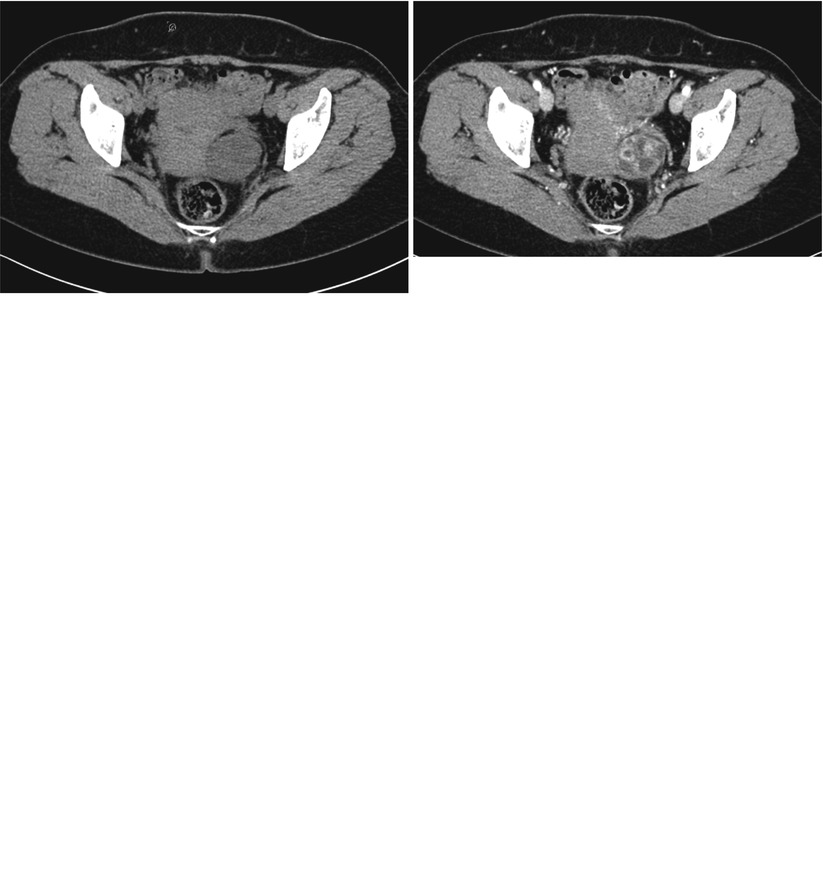
Fig. 22.9




Solitary fibrous tumor in the pelvic cavity. (a) On the non-contrast CT image, well-defined oval-shaped mass is seen in the left side of the uterus. (b) On the contrast-enhanced CT image, the mass manifests as heterogeneous enhancement with multifocal non-enhancing areas (arrowheads). (c) On the T1-weighted image, the mass manifests as an iso-signal intensity compared to the pelvic muscle. (d) On the T2-weighted image, the mass appears as intermediate high SI. The non-enhancing area on contrast-enhanced CT images shows high signal intensity, suggestive of cystic change (arrowheads). (e) On the contrast-enhanced T1-weighted image, the mass shows strong enhancement with non-enhancing areas of cystic change. This lesion was confirmed as solitary fibrous tumor
Related posts:
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
