Malignant Lesions
INVASIVE DUCTAL CARCINOMA
Invasive ductal carcinoma not otherwise specified (NOS), or no special type, is the most common type of breast cancer, representing 65% to 75% of mammary carcinomas (1,2). Patients may present with a hard, fixed, palpable mass that may cause skin thickening and retraction (Figure 7.1). When more advanced, breast cancer can deform the breast with a protruding, fungating (Figure 7.2), or ulcerating (Figure 7.3) mass. If the cancer develops close to the subareolar area, patients may describe progressive nipple inversion or retraction (Figure 7.4). Rarely, patients present with spontaneous nipple discharge, and less than 1% of patients present with metastatic disease to the axilla but no clinically or mammographically apparent primary lesion in the ipsilateral breast. In these patients, magnetic resonance imaging (MRI) may prove to be helpful in identifying the primary lesion (3).
Invasive ductal carcinomas, not otherwise specified, represent 65% to 75% of all diagnosed breast cancers.
With the increasing use of screening mammography, patients with invasive ductal carcinomas are diagnosed before signs of cancer are detected or symptoms have developed. A spiculated mass (Figure 7.5) is the most common mammographic finding in asymptomatic women. The mass may cause architectural distortion and have associated malignant-type calcifications indicating an associated intraductal component. Less commonly, invasive ductal carcinoma presents as a round or oval mass with well-circumscribed to ill-defined or indistinct margins (Figure 7.6A), focal parenchymal asymmetry (Figure 7.7), distortion (Figure 7.8), or diffuse changes (Figure 7.9). The density of the lesions is variable, and these masses can be low density (Figure 7.10).
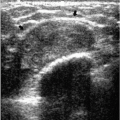
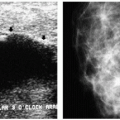
In many women, the mammographic features of a mass (e.g., spiculated with linear, casting-type calcifications) are such that an ultrasound does not add significant information. In these patients, ultrasound is done primarily to help direct the imaging-guided biopsy. In other patients, however, ultrasonography is helpful and compliments mammography in characterizing lesions. As discussed in Chapter 4, when a patient presents with a palpable mass and dense tissue is seen mammographically at the site of clinical concern, ultrasonography is critical in the characterization of the palpable abnormality (Figure 7.11). On ultrasound, an irregular, ill-defined hypoechoic mass is often imaged corresponding to the mass seen mammographically or palpated clinically. Spiculation, microlobulation, vertical orientation, angular margins, calcifications, extension of tumor into ducts pointing toward the nipple, and branching of tumor away from the nipple with variable amounts of shadowing are additional findings associated with malignancy (4). In patients with predominantly fatty tissue, and less commonly glandular tissue, the ultrasound study may be normal because the lesion is isoechoic to the surrounding tissue (Figure 7.11C, D). Many of our patients with invasive ductal carcinoma NOS presenting with a round mass (expansile margins), posterior acoustic enhancement and marked hypoechogenicity, have poorly differentiated, rapidly growing tumors (Figure 7.6B).
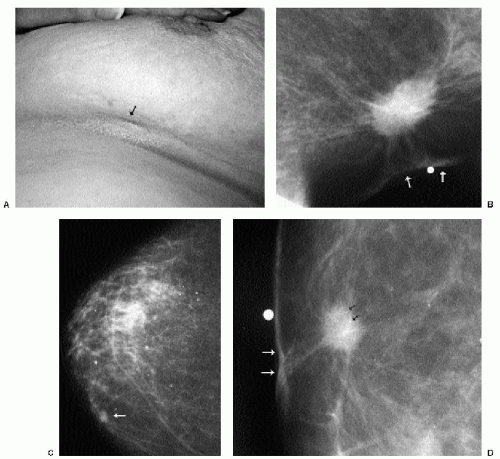 Figure 7.1 Well-differentiated, invasive ductal carcinoma, not otherwise specified. A. A 77-year-old patient presenting with dimpling (arrow) just above the inframammary fold on the left. In some patients, dimpling becomes apparent during compression. B. Spot tangential view taken at site of the dimpling. Spiculated mass with skin retraction and thickening (arrows). C. In an 84-year-old patient, the craniocaudal view identifies a mass (arrow) on the medial aspect of the right breast. D. Spot compression view demonstrates spiculated mass with associated calcifications (black arrows), skin thickening, and retraction (white arrows). |
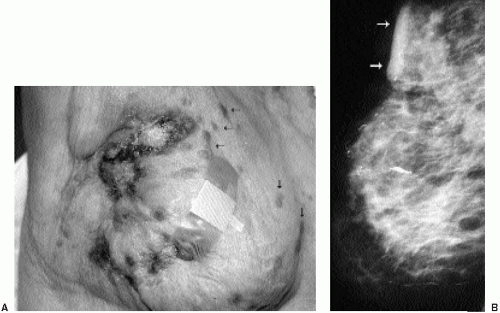 Figure 7.2 Poorly differentiated, invasive ductal carcinoma, not otherwise specified. A. A 97-year-old patient with advanced breast cancer. Marked deformity of the right breast is seen with ulceration. Small erythematous nodules (black arrows) represent skin metastases. B. Diffusely abnormal mammogram with decreased compressibility of the breast as well as skin and trabecular thickening. Prominent skin changes are noted at the site of ulceration (arrows). Some of the mammographic findings may be attributable to ipsilateral axillary adenopathy with resultant lymphatic obstruction. |
 Figure 7.3 Moderately differentiated invasive ductal carcinoma, not otherwise specified. A 78-year-old patient with ulceration (arrow) secondary to underlying advanced breast cancer. |
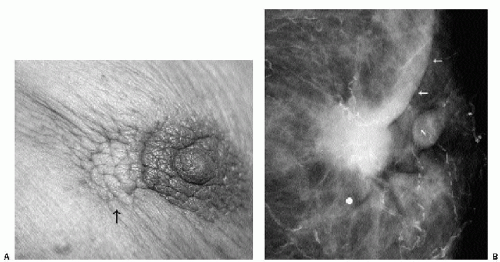 Figure 7.4 Moderately differentiated, invasive ductal carcinoma, not otherwise specified. A. A 90-year-old patient presenting with retraction and dimpling (arrow), left periareolar region. B. Spot compression view demonstrates ill-defined mass (metallic BB) with associated skin thickening and retraction (arrows) adjacent to the left nipple (N). Extensive arterial calcification is present. |
 Figure 7.5 Well-differentiated, invasive ductal carcinoma, not otherwise specified. Craniocaudal (CC) (A) and mediolateral oblique (MLO) (B) views in a 53-year-old patient. Screening mammogram. A possible mass (arrow) is detected medially on the left CC view. It is not definitely seen on the MLO view, however, it is suspected to be in the area just above the inframammary fold (arrow). Category 0: additional imaging evaluation is indicated. C. Spot compression view in the CC projection confirms the presence of a spiculated mass (arrow). D. Spot compression view in the MLO projection just above the inframammary fold demonstrates spiculated mass (infiltrative margins) in second projection (arrow). Category 4. Imaging-guided biopsy is undertaken using ultrasound (not shown) guidance. |
 Figure 7.5 (continued) |
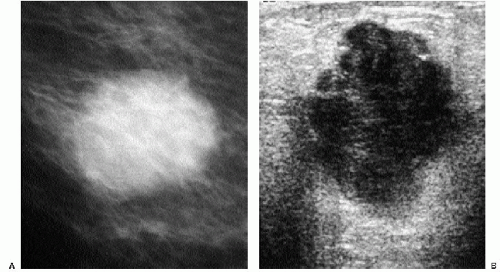 Figure 7.6 Poorly differentiated, invasive ductal carcinoma, not otherwise specified. A. A 45-year-old patient. Round mass with indistinct margins (expansile margins). B. Mass with heterogeneous echotexture; lobulated, angulated, ill-defined margins; and posterior acoustic enhancement. In our experience, many patients presenting with a round or oval mass (expansile margins) having posterior acoustic enhancement and marked hypoechogenicity are diagnosed with poorly differentiated, rapidly growing invasive ductal carcinoma. C. In the ipsilateral axilla, enlarged lymph nodes are imaged, characterized by a bulging cortex (black arrows), marked hypoechogenicity, complete loss or attenuation (mass effect) of the central fatty hilum (white arrow), and posterior acoustic enhancement. D. Third node in axilla: enlarged, nearly anechoic with posterior acoustic enhancement (simulates a cyst) and marked attenuation of the fatty hilum (arrow). Breast primary and metastatic disease to axillary lymph node diagnosed on imaging-guided core biopsies. Patient treated with neoadjuvant therapy followed by surgery. |
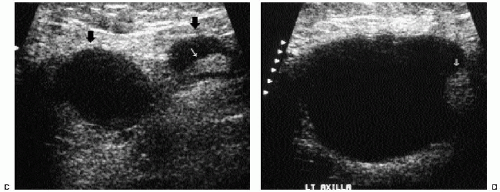 Figure 7.6 (continued) |
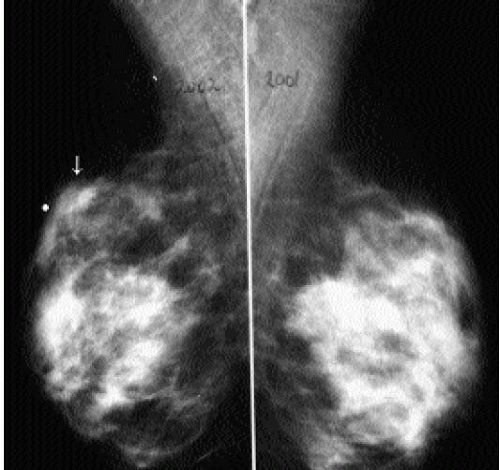 Figure 7.7 Moderately differentiated, invasive ductal carcinoma, not otherwise specified. A. Right mediolateral oblique views from 2002 and 2001 back to back. Patient presents with a lump in the right breast (metallic BB marks area). Focal parenchyma asymmetry (arrow) is developing compared with previous study and corresponds to area of clinical concern. Palpable areas of focal parenchymal asymmetry require spot compression views, correlative physical examination, and ultrasound evaluation. |
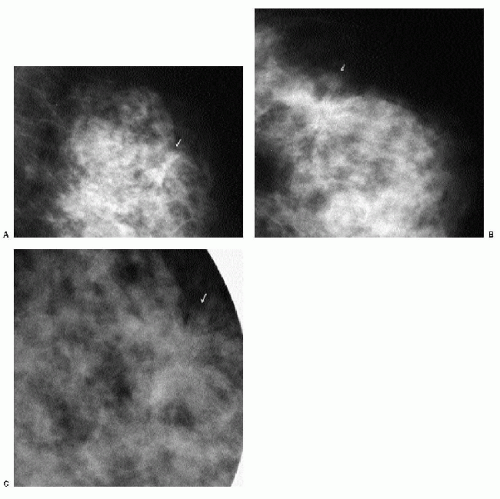 Figure 7.8 Moderately differentiated, invasive ductal carcinoma, not otherwise specified. Mediolateral oblique (A) and craniocaudal (B) views. Screening study in a 52-year-old patient. Possible distortion is noted (arrows). As discussed for calcifications, detection of these areas in a background of dense tissue requires a specific search for distortion. Category 0: additional imaging evaluation is indicated. C. Spot compression and rolled views (only one shown) confirm the presence of distortion (arrow). Note straight lines at arrow tip. Category 4. Imaging-guided biopsy is undertaken under ultrasound (not shown) guidance. |
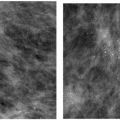
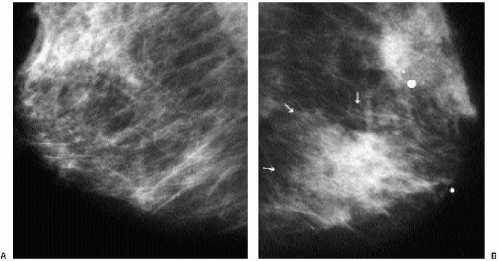 Figure 7.9 Well-differentiated, invasive ductal carcinoma with associated intermediate-grade ductal carcinoma in situ. Right (A) and left (B) mediolateral oblique views in a 67-year-old patient presenting with a palpable, global area of parenchymal asymmetry in the left breast. This breast is less compressible than the right and is perceived as smaller. Diffuse changes, with a global area of parenchymal asymmetry (arrows), are imaged at the palpable site (metallic BB). |
 Figure 7.10 Moderately differentiated, invasive ductal carcinoma, not otherwise specified. A. Mediolateral oblique view in a 71-year-old patient. Low-density, round mass (arrow) is identified as new compared with the prior study. Category 0: incomplete; additional imaging evaluation is indicated. B. Spot compression views confirm the presence of a low-density mass (orthogonal view not shown) with indistinct margins. Category 4: biopsy is indicated. Although more commonly high in density, breast cancer can be low in density. C. Ill-defined, hypoechoic mass (arrows) with associated shadowing corresponding to the mammographic finding. Incorporating information from prior studies, spot compression views, physical examination, and ultrasound is helpful in determining appropriate recommendations. Imaging-guided biopsy is undertaken. |
 Figure 7.10 (continued) |
 Figure 7.11 Moderately differentiated invasive ductal carcinoma, not otherwise specified (NOS). A. Mediolateral oblique (MLO) view in a 37-year-old patient presenting with a palpable mass; metallic BB marks the area. MLO and spot views (not shown) demonstrate dense glandular tissue. On physical examination, a hard mass is readily palpated at the site of concern to the patient. B. Irregular, hypoechoic mass (arrow) with angular margins is imaged corresponding to the area of clinical concern. Imaging-guided biopsy is done. In patients with a discrete palpable abnormality and dense tissue mammographically, ultrasound is indicated for further evaluation. C. Different patient with poorly differentiated invasive ductal carcinoma, NOS. Craniocaudal view demonstrates oval mass (arrow) in medial aspect of the breast. D. Spot compression view confirms oval mass with indistinct margins. Seemingly normal tissue is seen on ultrasound. Because no cyst is imaged, it is presumed that the mass seen mammographically is solid and isoechoic with surrounding tissue. Stereotactically guided biopsy is done to establish the diagnosis. |
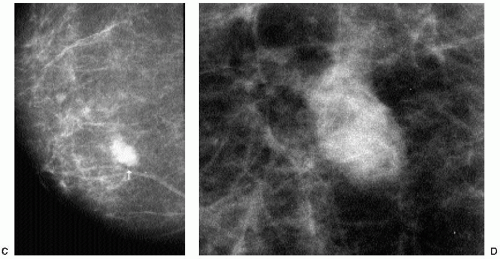 Figure 7.11 (continued) |
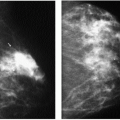
It is important to recognize that patients with breast cancer are at significantly higher risk for other lesions. Multifocal lesions are defined as multiple cancers occurring in the same quadrant (Figure 7.12), whereas multicentric cancers are those occurring in different quadrants of the involved breast. Bilateral cancers are synchronous (Figure 7.13) when diagnosed at the same time, or within 6 months of each other, and metachronous (Figure 7.14) when they occur bilaterally at different times (diagnosed more than 6 months apart). The reported frequency of multifocality varies, depending on study design and meticulousness of histologic evaluation, and may be as high as 33% to 50% (5,6).
Dynamic contrast-enhanced MRI is emerging as a powerful tool that, when used in conjunction with mammography and ultrasound, can help establish the presence of clinically occult multifocal and multicentric disease.
 Figure 7.12 Multifocal, poorly differentiated invasive ductal carcinoma with associated highnuclear-grade ductal carcinoma in situ. In a 67-year-old patient, a spot compression view demonstrates three masses with ill-defined margins and associated linear (casting) calcifications (arrows) consistent with the diagnosis of multifocal (same quadrant) invasive ductal carcinoma with associated intraductal carcinoma. Multicentricity is suggested when lesions highly suggestive of cancer are seen in separate quadrants. |
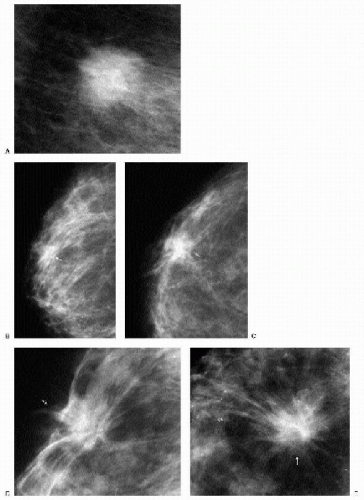 Figure 7.13 Synchronous lesions, invasive ductal carcinomas, not otherwise specified; moderately and well-differentiated left and right breast, respectively. A. Left breast. Mediolateral oblique spot compression view demonstrates mass with ill-defined margins. Having detected one lesion, keep looking! Remember that these patients are at increased risk for multifocal, multicentric, and bilateral disease. Mediolateral oblique (B) and craniocaudal (C) views of the right breast (only anterior portion of breast is shown). Anterior tissue is not well compressed, and there is the suggestion of “straight lines” (arrows). With what degree of certainty would you say there is a lesion at this site? Mediolateral oblique (D) and craniocaudal (E) spot compression views greatly simplify the situation. These demonstrate a spiculated mass (arrows). Bilateral ultrasound-guided (not shown) core biopsies are done. |
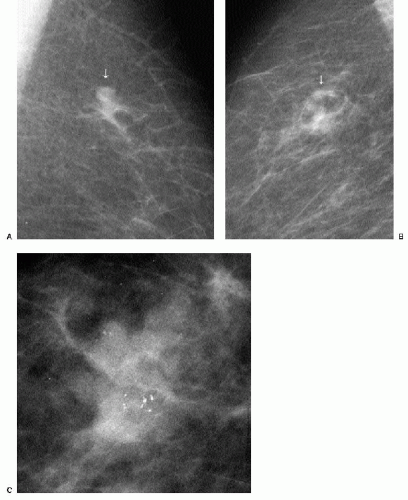 Figure 7.14 Metachronous lesions, invasive ductal carcinoma, not otherwise specified. A. Mediolateral oblique view, left breast. Screen-detected mass (arrow). Invasive ductal carcinoma diagnosed. B. Mediolateral oblique (MLO) view, right breast, 3 years after image in part A. New area of focal asymmetry (arrow) with possible calcifications. Category 0: additional imaging evaluation is needed. C. Double spot compression magnification views (only MLO view shown) confirm the presence of an irregular mass with associated calcifications. In patients with a history of breast cancer, aggressively pursue any perceived changes in the contralateral breast. In this patient, the second lesion is arising within tissue and has associated ductal carcinoma in situ consistent with second primary and not metastasis from the prior cancer. |
The described frequency of synchronous lesions is 0.1% to 2%, compared with 1% to 12% for metachronous lesions. The risk for subsequent breast cancer development among patients with a history of breast cancer is significant, and some of the factors to consider
in assessing this risk are listed in Box 7.1. In the general population, 0.1% of women per year are expected to develop breast cancer. In comparison, the frequency of developing a second breast cancer among patients with a history of breast cancer is 0.53% to 0.8% per year (6). Nielsen and colleagues reported on 86 women with a diagnosis of invasive ductal carcinoma, in whom, at autopsy, invasive and in situ lesions were identified in the contralateral breast in 33% and 35% of patients, respectively (7). In a separate study done by the same investigators in an age-matched population, autopsy results identified 14 patients with in situ lesions and only 1 patient with invasive cancer among 77 women with no history of breast cancer (8).
in assessing this risk are listed in Box 7.1. In the general population, 0.1% of women per year are expected to develop breast cancer. In comparison, the frequency of developing a second breast cancer among patients with a history of breast cancer is 0.53% to 0.8% per year (6). Nielsen and colleagues reported on 86 women with a diagnosis of invasive ductal carcinoma, in whom, at autopsy, invasive and in situ lesions were identified in the contralateral breast in 33% and 35% of patients, respectively (7). In a separate study done by the same investigators in an age-matched population, autopsy results identified 14 patients with in situ lesions and only 1 patient with invasive cancer among 77 women with no history of breast cancer (8).
Box 7.1: Factors to Consider in Assessing Risk for Subsequent Breast Cancer Development in Patients with Personal History of Breast Cancer
Tumor size
Degree of anaplasia
Location
Clinical stage
Family history
Multicentricity
Ductal carcinoma in situ
Premenopausal (younger patients)
Genetics: BRCA1 and BRCA2
Peutz-Jeghers syndrome
Histology of lesion (greater incidence with tubular or invasive lobular carcinomas)
When a patient with breast cancer develops a lesion in the contralateral breast, the second lesion may represent a second primary or a metastasis from the prior lesion (6). In considering prognosis and treatment options for the patient, it is important to distinguish between these two considerations (Figure 7.14). The features suggestive of a second primary are contrasted with the features suggestive of metastatic disease in Table 7.1.
In women with known invasive breast primary tumors, we routinely scan the ipsilateral axilla. Ultrasound evaluation in patients with suspected axillary adenopathy can be useful because it provides access to an area that may be difficult to evaluate mammographically. Ultrasonographic features of axillary lymph nodes that raise our concern include marked hypoechogenicity (in some patients, nearly anechoic) with through transmission, bulging cortex, mass effect, attenuation or obliteration of the
hyperechoic fatty hilum (Figure 7.6C, D), and increased blood flow. If a suspicious node is identified, a core biopsy or fine-needle aspiration is done at the time of the primary breast lesion biopsy. Patients identified with metastatic disease bypass sentinel lymph node biopsy and go on to have full axillary dissections at the time of the lumpectomy. When an abnormal intramammary lymph node is identified and found to be positive for metastatic disease, consider preoperative wire localization of the intramammary lymph node. These nodes are not routinely excised during axillary dissections.
hyperechoic fatty hilum (Figure 7.6C, D), and increased blood flow. If a suspicious node is identified, a core biopsy or fine-needle aspiration is done at the time of the primary breast lesion biopsy. Patients identified with metastatic disease bypass sentinel lymph node biopsy and go on to have full axillary dissections at the time of the lumpectomy. When an abnormal intramammary lymph node is identified and found to be positive for metastatic disease, consider preoperative wire localization of the intramammary lymph node. These nodes are not routinely excised during axillary dissections.
Table 7.1: Features of Second Primary Tumor Compared with Metastasis from Contralateral Breast | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Histologically, invasive ductal carcinomas, NOS, demonstrate variable growth patterns (infiltrative, expansile), cellular morphology, and no special features. Several grading systems are available based on tubule formation, nuclear morphology, and mitotic activity. Estrogen receptors are reportedly positive in 55% to 72% of lesions; however, poorly differentiated lesions are less likely to have estrogen receptors. Progesterone receptors occur in 33% to 70% of lesions, and about 15% of lesions are estrogen receptor positive and progesterone receptor negative (1,2,6).
EXTENSIVE INTRADUCTAL COMPONENT
Patients with invasive ductal carcinomas and extensive areas of associated intraductal carcinoma were initially thought to have a worse prognosis and were described as having a higher incidence of local recurrence after conservative treatment. This is probably related to incomplete resection of the lesion and residual disease in the breast (9). When lesions with an extensive intraductal component (EIC) are adequately resected, prognosis is not significantly different from that of women with lesions lacking EIC (10,11). When malignant-type calcifications are seen extending for a distance away from a clinically or mammographically detected mass (Figure 7.15), it is important to alert the surgeon
and localize the area (bracketing may be needed) so that the intraductal disease is resected with the invasive component. Definitions of EIC have varied. Currently, EIC is diagnosed when ductal carcinoma in situ (DCIS) constitutes 25% or more of the invasive tumor or when DCIS is present within and extends beyond the invasive component (1,2,6,12).
and localize the area (bracketing may be needed) so that the intraductal disease is resected with the invasive component. Definitions of EIC have varied. Currently, EIC is diagnosed when ductal carcinoma in situ (DCIS) constitutes 25% or more of the invasive tumor or when DCIS is present within and extends beyond the invasive component (1,2,6,12).
 Figure 7.15 Invasive ductal carcinoma, not otherwise specified, with associated high-nuclear-grade ductal carcinoma in situ (e.g., extensive intraductal component). A 55-year-old patient. When a mass is seen with associated pleomorphic and linear calcifications, an invasive ductal carcinoma (the mass) with an associated intraductal component (the calcifications) is the likely diagnosis. If extending away from the mass, it is important that the extent of the calcifications be determined with appropriate magnification views and that this be communicated to the surgeon and pathologist. Localization of the calcifications may be indicated for adequate excision.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|