Fig. 7.1
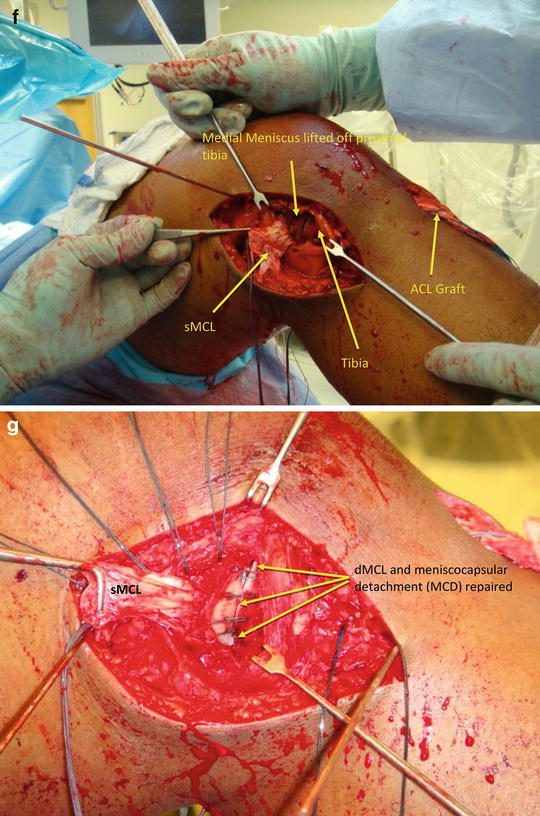
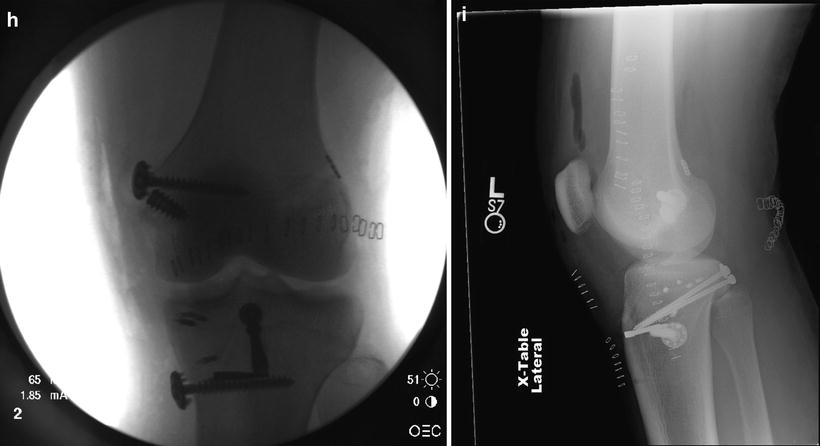
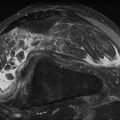
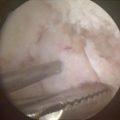
(a) Valgus stress radiograph demonstrating medial compartment opening consistent with a complete MCL injury. (b) Coronal MRI demonstrating a distal MCL injury with displacement into the joint. (c) Stress radiograph demonstrating a PCL injury. Note posterior displacement of the tibia in relation to the femoral condyles. Compare with (d) which shows the contralateral normal side. (e) Arthroscopic view demonstrating displacement of the MCL into the knee. (f) Operative view showing superficial MCL (forceps) after extraction from the joint. (g) Deep repair of medial meniscus (distally) and deep MCL (proximally). Superficial MCL is in a right angle clamp proximally. HI. AP (h) and lateral radiographs (i) demonstrating MCL repair/reconstruction (and PCL inlay reconstruction)
Figure 7.1d shows a T2-weighted coronal sequence MRI of the left knee demonstrating complete disruption of the sMCL from the tibial insertion. The dMCL is also ruptured from its tibial attachment with a residual wisp of ligament clearly visible on the medial tibia. The medial meniscus is extruded and elevated superiorly with the intact femoral portion of the dMCL. The tibial portion of the sMCL can be seen incarcerated in the joint inferior to the medial meniscus. A bone bruise is also seen on the lateral femoral condyle. Additional MRI sequences (not shown) revealed a rupture of the ACL and PCL.
Arthroscopy
Arthroscopic exam confirmed the presence of an ACL and PCL rupture. Figure 7.1e shows an arthroscopic picture taken from the inferolateral portal looking into the medial compartment. A “meniscus rise” sign [6] is present due to complete rupture of the tibial portion of the dMCL. In addition, the tibial portion of the sMCL can be seen flipped into the joint underneath the medial meniscus.
The ACL was reconstructed arthroscopically with a semitendinosus and gracilis autograft from the ipsilateral side. The PCL was reconstructed using a posterior tibial inlay technique with bone-patellar tendon-bone (BPTB) autograft from the ipsilateral side.
A separate medial incision centered just posterior to the midline of the knee joint was made running longitudinally from the adductor tubercle to a point 7–8 cm passed the joint line distally. As expected, the sMCL was completely ruptured from its tibial attachment and flipped into the joint between the medial tibial plateau and medial meniscus. The medial meniscus was separated from the overlying capsule along its posterior portion. The dMCL was still attached to the medial meniscus and avulsed from the proximal medial tibia. Figure 7.1f is an intraoperative photo showing the tibial portion of the sMCL after it has been freed from the knee joint. Though subtle, space can be seen beneath the medial meniscus with the tibial portion of the dMCL still attached and projecting posteromedially. Figure 7.1g shows the medial meniscus and tibial portion of the dMCL after repair with three suture anchors. The sMCL is flipped up proximally with sutures in it for planned repair. The semimembranosus tendon was intact, but in addition to the posteromedial meniscocapsular detachment (MCD), the POL was torn from the tibia, and it is expanded onto the semimembranosus. The meniscocapsular detachment and tibial portion of the dMCL were repaired primarily with three suture anchors along the medial tibial margin. The sMCL was then repaired primarily back to the tibial surface utilizing suture anchors. Tibial sided avulsion injuries heal less predictably than femoral sided avulsion injuries, so the decision was made to augment or repair with semitendinosus allograft, which we would also use to reconstruct the posteromedial corner, namely, the ruptured POL. The isometric point of the femoral origin of the sMCL was identified with fluoroscopic guidance by drawing an imaginary line tangential to the posterior femoral cortex and to Blumensaat’s line horizontally. The MCL origin sits just proximal to the horizontal line and just posterior to the posterior femoral cortex line [9]. A guidewire was placed and the sMCL was attached both proximally and distally with a 6.5 mm screw and soft tissue washer construct. The sMCL is looped around the semimembranosus prior to attachment as has been described by Stannard [1].
Postoperative images are seen in Fig. 7.1h, i.
Discussion Points
General imaging findings with MCL ruptures
Anatomy of the superficial and deep MCL
The role of the PMC in knee stability and techniques for reconstruction
Allograft augmentation of the MCL and PMC in the setting of multiligament knee injuries
Case 2
History
The patient is a 20-year-old football wide receiver at the collegiate level. He sustained a noncontact external rotation, axial load, and valgus injury to his right knee after landing with a caught football at an awkward position. He presents to our surgery center 2 weeks after the injury.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


