Fig. 21.1
(a) Three-dimensional surface-rendering ultrasound of the fetal face shows cleft lip, a large polyp protruding through the right nostril, two nasal dorsal polyps, and a left cheek skin tag. (b) Same view as in (a) with open mouth for a better depiction of the median upper lip cleft
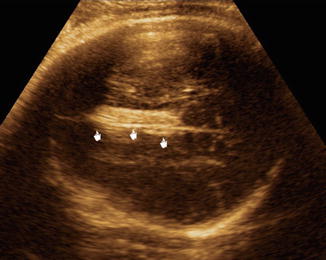
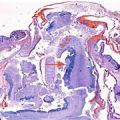
Fig. 21.2
Axial two-dimensional ultrasound image of the fetal head shows an echogenic mass in the interhemispheric fissure representing a lipoma
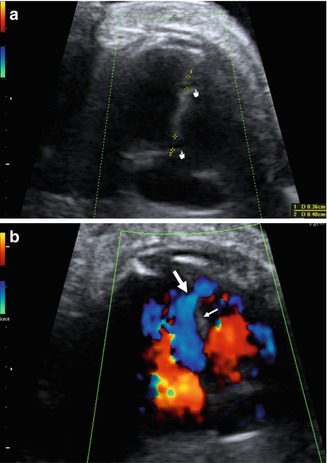
Fig. 21.3
(a) Four-chamber view in B-mode depicts two small ventricular septal defects (denoted by calipers). (b) Color Doppler ultrasound shows flow through the muscular ventricular septal defect (arrow). Small arrow denotes the septum
Given the fetal phenotypic features, the diagnosis of Pai syndrome was made and confirmed after birth (Fig. 21.4a). The newborn infant had no major neonatal complications. Initial feeding problems were managed with a palatal obturator. Postnatal karyotype was reported as normal. Repair of the cleft lip and excision of the polyp were performed during the neonatal period. In a subsequent operation, the palate was surgically reconstructed. The small ventricular septal defects spontaneously closed during the first year of age. Figure 21.4b shows the postoperative results at the age of 3 years. The infant is currently 5 years of age and her neurodevelopmental assessment has been reported as normal.
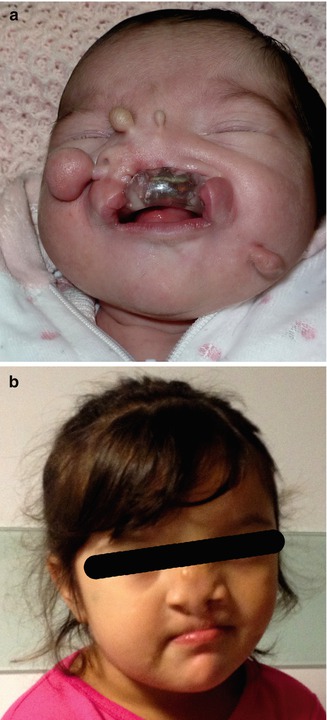
Fig. 21.4
(a) Photograph of the newborn infant shows the facial features of Pai syndrome. The nasal polyp protruding from the right nostril and the skin tags are clearly seen. The palate obturator, used for feeding purposes, prevents full view of the cleft lip and palate. (b) Follow-up at 3 years of age shows the postoperative results (a, b published with permission from the parents)
21.3 Discussion
Pai syndrome is a rare disorder first described by Pai et al. in 1987 in a female newborn that presented with clefting of the upper lip, nasal skin polyps, and midline lipoma of the brain [1]. As an isolated finding, median clefting of the upper lip is rare. However, this condition may be related to several syndromes [4]. The nasal polyps are considered the hallmark of Pai syndrome and the most common site of presentation is the nasal septum that gives rise to polyps arising through the nostrils. The columella is the second most common site; rare locations are the dorsum/bridge and tip of the nose [5]. Usually, these polyps are hamartomas (lipomas and myolipomas) [5, 6].
After the original description of this syndrome, several cases characterized by median facial cleft without cleft palate, nasal or facial polyps, or brain interhemispheric lipomas have been reported. Therefore, minimum diagnostic criteria for Pai syndrome have been established: one or more hamartomatous nasal polyps plus a median cleft lip (with or without cleft alveolus or palate) and/or mid-anterior alveolar process congenital polyp [5]. As pericallosal lipoma was reported in 85 % of the cases that underwent brain imaging, this feature has also been proposed as an additional criterion [3].
Interhemispheric/pericallosal lipomas have typical ultrasound features that make them very easy to identify during prenatal ultrasound in the majority of cases [7]. As there is no adipose tissue in the brain, lipomas of the central nervous system are presumed to arise from the primitive meninx descending into the interhemispheric fissure during cleavage of the prosencephalic vesicle [8]. At this location, the lipoma may interfere with corpus callosum development [7]; therefore, complete/partial agenesis or hypoplasia of the corpus callosum is a frequently associated finding [5, 7, 9]. Other developmental anomalies of the craniofacial region that are included in the clinical spectrum of Pai syndrome are bifid nose, bifid uvula, double frenulum, midline sinus, median alveolar cleft, and ocular hypertelorism. Occasionally, ophthalmic abnormalities of the iris and cornea, like coloboma, microcornea, or lenticonus, have been also reported [2, 3, 8]. DeMyer [10] stated that median cleft of the upper lip is associated with orbital hypertelorism and five other facial defects: V-shaped frontal hairline, cranium bifidum occultum, primary telecanthus, median cleft of the premaxilla, and median cleft palate.
Related posts:
 Congenital Subcutaneous Mixed Venous-Lymphatic Orofacial Malformation Associated with Macroglossia: Prenatal Diagnosis with Ultrasound and Fetal MRI
Congenital Subcutaneous Mixed Venous-Lymphatic Orofacial Malformation Associated with Macroglossia: Prenatal Diagnosis with Ultrasound and Fetal MRI
 The Genetics of Facial Cleft
The Genetics of Facial Cleft
 Acromelic Frontonasal Dysplasia (Median Cleft Face Syndrome)
Acromelic Frontonasal Dysplasia (Median Cleft Face Syndrome)
 The Fetal Brain in Fetuses with Orofacial Abnormalities
The Fetal Brain in Fetuses with Orofacial Abnormalities
 Magnetic Resonance Imaging (MRI) in the Evaluation of the Fetal Face
Magnetic Resonance Imaging (MRI) in the Evaluation of the Fetal Face
 The Role of 2D/3D/4D Ultrasound in the Prenatal Assessment of Cleft Lip and Palate
The Role of 2D/3D/4D Ultrasound in the Prenatal Assessment of Cleft Lip and Palate
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


