(1)
Department of Radiology, John H Stroger Jr Hospital of Cook County, Chicago, IL, USA
Lymphoma
Imaging Features
1.
Hilar and mediastinal lymphadenopathy
2.
Multiple pulmonary nodules
3.
Interstitial and alveolar infiltrates and pleural effusion
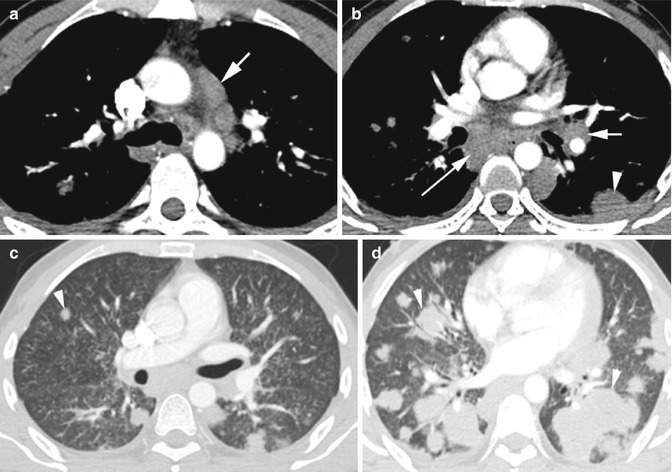
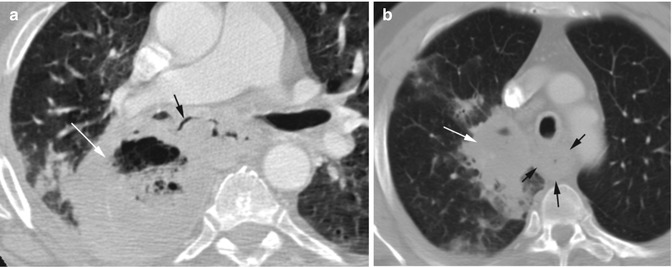
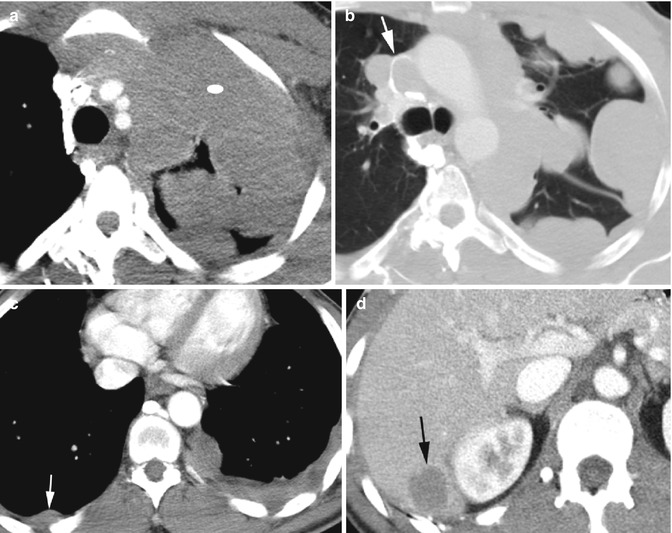
Fig. 10.1
Lymphoma with histoplasma infection in a HIV/AIDS patient. Axial CT (a) shows enlarged lymph nodes in the mediastinum (arrow), (b) enlarged lymph nodes in the left hilum (short arrow) and mediastinum (long arrow), and pleural-based nodule (arrowhead). (c) Diffuse centrilobular micronodules are seen bilaterally with subpleural sparing. Solid lung nodule (arrowhead) and pleural-based masses bilaterally. (d) Many of the large solid masses (arrowhead) in the parenchyma are seen more at the lung bases
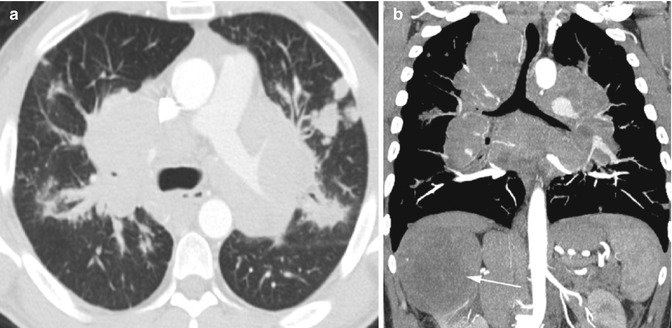
Fig. 10.2
Mediastinal and hilar LAD due to metastasis from RCC. (a, b) Axial and coronal reformatted CT show large lymph nodes in the bilateral hila and mediastinum narrowing in bilateral bronchi and with multiple solid lung nodules. A large necrotic right renal mass is seen (arrow)
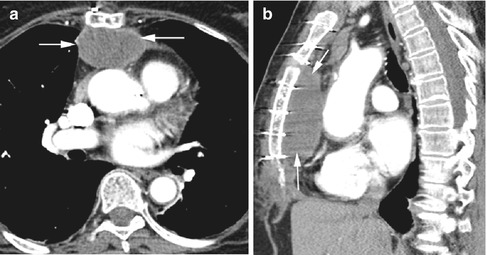
Fig. 10.3
Hematoma in the anterior mediastinum post-surgery. (a, b) Axial and sagittal reformatted images show a large well-marginated retrosternal hematoma (arrows) with sternotomy sutures
Thyroid Lesions
Diagnosis
Goiter
Imaging Features
1.
Enlarged one or both lobes of the thyroid.
2.
Nodules solid, low density, or mixed.
3.
Calcifications can be coarse or microcalcification.
4.
Cystic lesions.
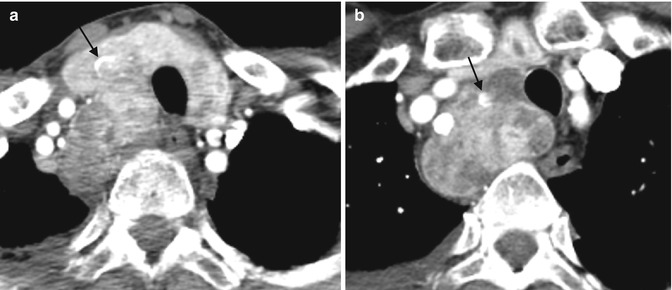
Fig. 10.4
Multinodular goiter with colloid cysts, biopsy proven. Axial CT (a, b) shows multiple low-density nodules bilaterally and retrosternal extension on the right side. Coarse calcifications is seen in the right lobe (arrow)
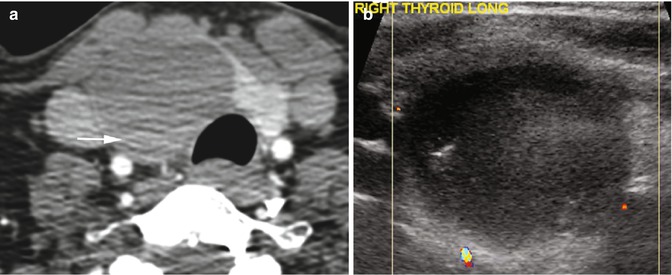
Fig. 10.5
Hemorrhage in a colloid cyst. (a) Axial CT shows a large cyst in the right lobe of the thyroid with dependent high-density hemorrhage (arrow). (b) Color Doppler US shows low-level echoes within the cyst in the right lobe of the thyroid with no internal vascularity and no increased vascularity of the cyst wall
Diagnosis
Thyroid Carcinoma
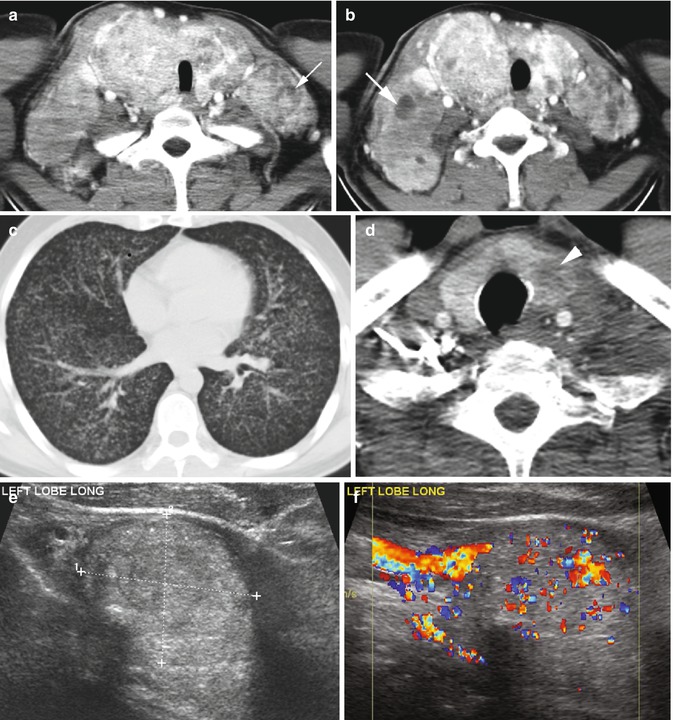
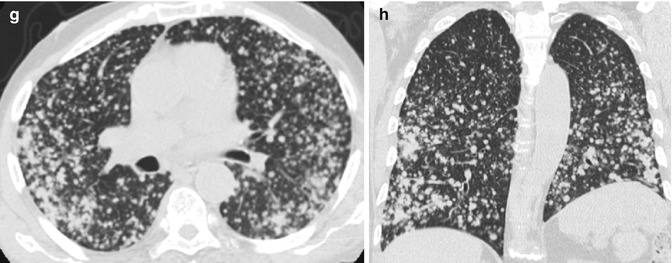
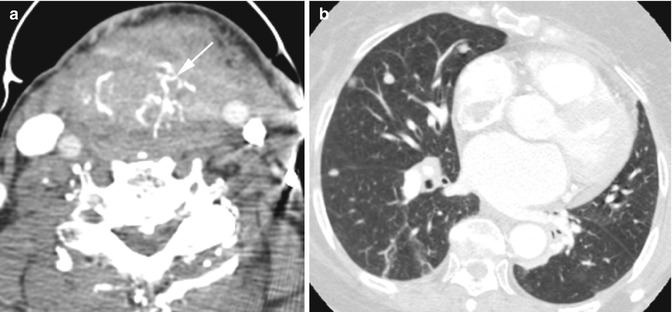
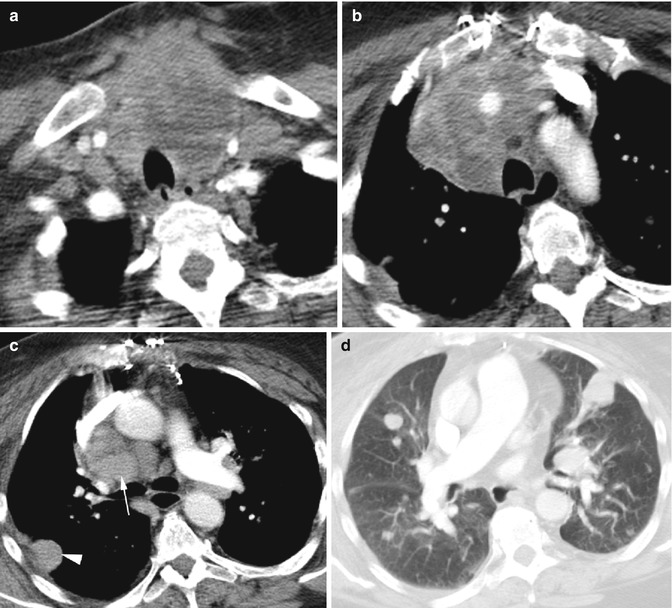
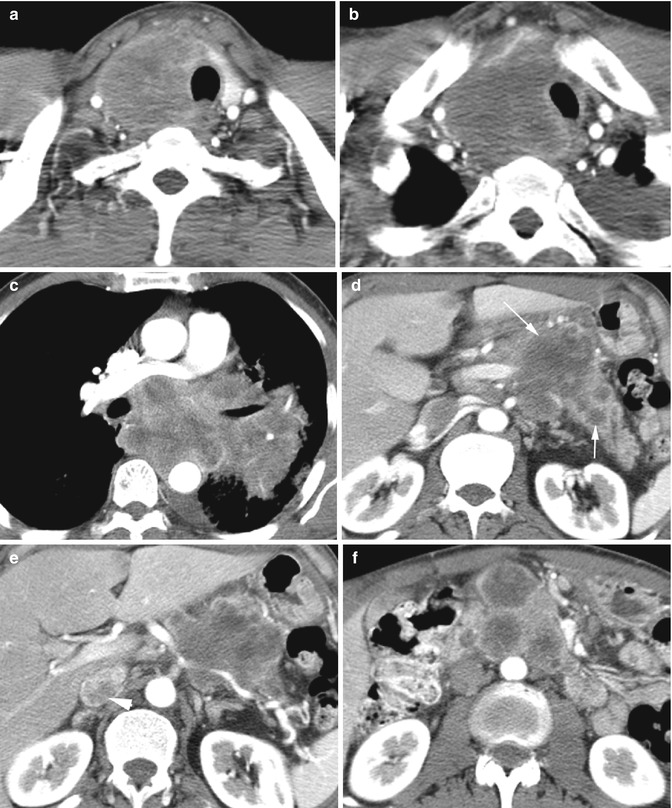
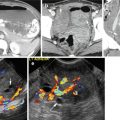
Fig. 10.6
Papillary thyroid cancer with pulmonary metastasis. Patient 1: (a, b) Axial CT neck shows both lobes of the thyroid to be enlarged, with increased vascularity and with multiple low-density foci. Low-density metastases are also seen in adjacent lymph nodes (arrows) bilaterally. (c) Axial CT of the chest shows miliary metastasis. Patient 2: (d) axial CT of the neck shows a small low-density ill-marginated nodule in the left thyroid lobe (arrowhead). (e, f) Grayscale and color Doppler ultrasound show hypervascular large heteroechoic solid mass (calipers in e) in the left lobe of the thyroid. (g, h) Axial and coronal reformatted CTs show macronodular metastasis to bilateral lungs
Fig. 10.7
Hurthle cell follicular thyroid carcinoma. Axial CT (a) of the neck shows coarse calcifications (arrow) in the diffusely enlarged thyroid. (b) Axial CT of the chest shows nodular metastases in the lungs (b)
Fig. 10.8
Anaplastic thyroid carcinoma with lung metastasis. Axial CT (a, b) shows diffuse enlargement of both lobes of the thyroid with irregular low densities and with retrosternal extension of the right lobe. (c) Lymphadenopathy is seen at the precarinal region (arrow) and in the left hilum, and pleural-based metastasis is seen in the right lung (arrowhead). (d) Axial CT of the lung windowing at lower level shows multiple large solid lung metastases
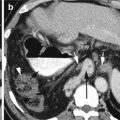
Fig. 10.9
Small cell lung cancer with metastasis to the thyroid, pancreas, adrenal gland, and mesenteric root lymph nodes. Axial CT of the chest (a, b) shows low-density metastasis to the right lobe of the thyroid. (c) Shows lung carcinoma in the left hilum extending into the mediastinum and shows narrowing of the left upper lobe of the bronchus. Axial CT of the abdomen (d–f) shows multiple low-density metastases to the body and tail of the pancreas (arrows) and right adrenal gland (arrowhead). (f) Necrotic lymph nodes at the root of mesentery
Thymic Tumors
Diagnosis
Thymic Epithelial Tumors
Imaging Features
Thymoma
1.
Most are encapsulated solid lesions that can be oval, round, or lobulated.
2.
Can have hemorrhage, necrosis, or cystic component.
3.
Calcification may be in the capsule or throughout the mass.
4.
Usually slow growing but can be aggressive and invade into the mediastinum, pleura, and pericardium.
Thymic carcinomas

1.
More aggressive and invades adjacent structures
2.
Calcification is more frequent and have low-density areas
3.
Distant metastasis and mediastinal lymphadenopathy
Fig. 10.10
Thymoma. (a–c) Axial CT of the mediastinum shows nonaggressive anterior mediastinal focal mass in three patients all with histologic diagnosis of benign thymoma. (c) Spindle cell benign thymoma
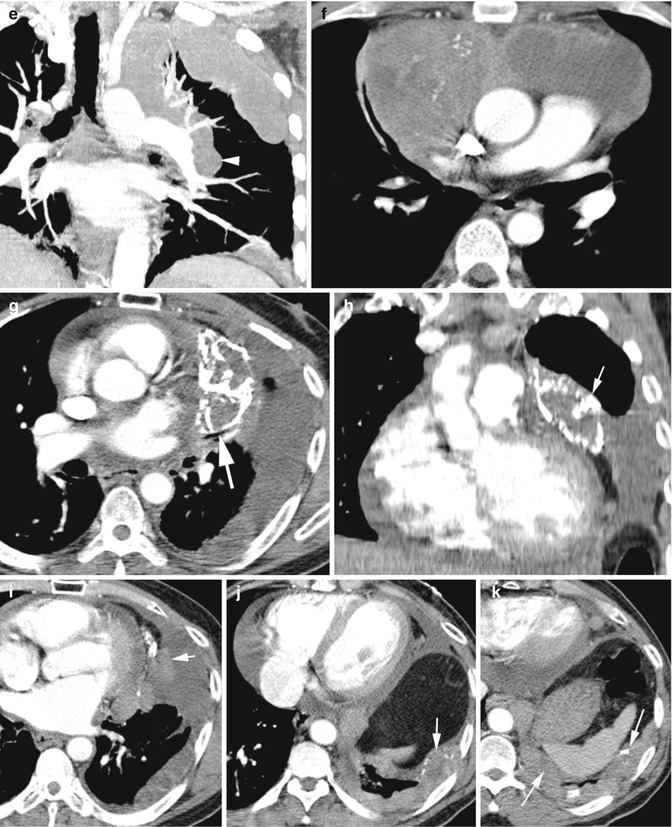
Fig. 10.11
Thymic carcinoma of three patients. Patient 1: (a–e) Axial and coronal reformatted CT show left anterior mediastinal mass (ellipse in a) infiltrating the pleura in the left thorax giving it a nodular appearance and with left hilar lymphadenopathy (arrowhead e). It is also compressing the superior vena cava (white arrow in b). Pleural metastasis is seen on the right side (white arrow in c) and to the liver (black arrow in d). Patient 2: (f) axial CT shows anterior mediastinal mass with calcification and areas of cystic degeneration. Patient 3: (g–k) axial and coronal reformatted CT show recurrence of thymic carcinoma with prior history of radiation therapy. Now shows curvilinear calcification of thymic mass (arrows in g, h) and pleural metastasis with similar calcification (arrows j, k). The mass shows invasion to the mediastinal pleura (arrow in i)
Diagnosis
Thymic Neuroendocrine Tumor
Imaging Features
1.
Lack fibrous capsule but commonly have necrosis or hemorrhage and may have fine calcification
2.
Invade to adjacent structures
3.
Distant intrathoracic and extrathoracic metastasis
4.
Difficult to differentiate from thymic epithelial tumors
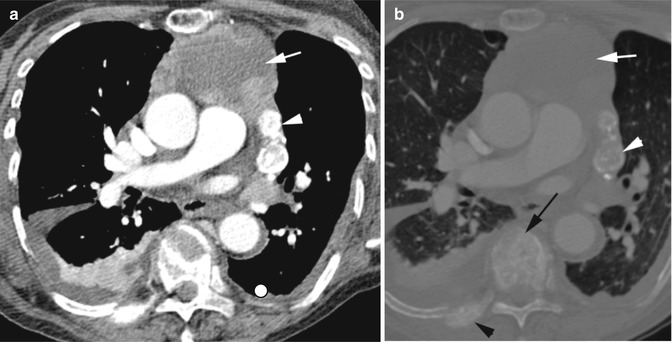
Fig. 10.12
Neuroendocrine tumor of the thymus with bony metastasis. (a, b) Axial CT shows a large anterior mediastinal mass with peripheral enhancement (white arrows), central necrosis, and coarse calcification (white arrowhead) with extension to the left hilum. Mixed metastasis is seen in the right posterior rib (black arrowhead) and to multiple vertebral bodies (only one shown, black arrow)
Diagnosis
Thymic Lymphoma
Imaging Features
1.
Enlarged single or multiple masses mimic other thymic lesions
2.
Difficult to distinguish from other thymic masses
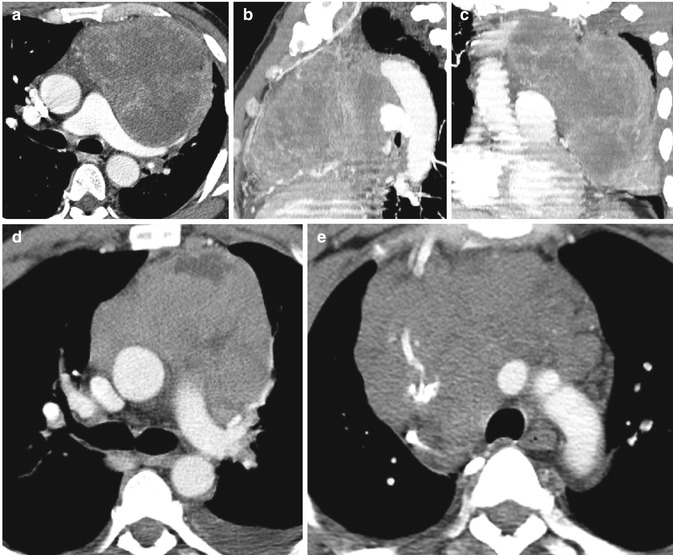
Fig. 10.13
Lymphoma in different patients. (a–c) B-cell lymphoma axial, sagittal, and coronal CT. (d) T-cell lymphoma axial CT. (e) Hodgkin’s lymphoma axial CT
Diagnosis
Thymic Germ Cell Tumor
Imaging Features
1.
Large lobulated anterior mediastinal mass.
2.
Seminomas are relatively homogenous.
3.
Teratomas may have one or more components of the embryonic germ cell layers.

Fig. 10.14
Thymic teratoma. Axial CT shows a large anterior mediastinal mass causing leftward deviation of the mediastinum and partial collapse of the right lung. The mass shows focal area of fatty tissue (white arrow), calcification (black arrow), and fluid collection (arrowhead)
Nongonadal Germ Cell Tumor
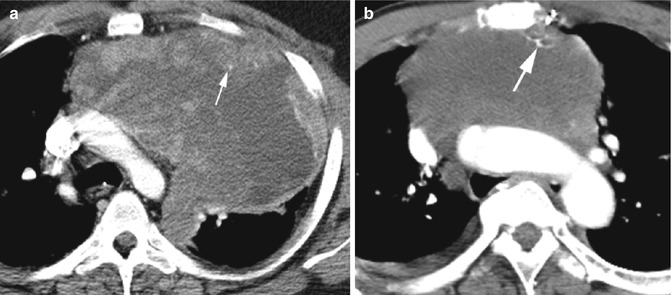
Fig. 10.15
Nongonadal seminoma in two patients. Axial CT (a) shows a large anterior mediastinal mass with low-density necrotic areas, enhancing solid tissue, and small specks of calcification (arrow). (b) Small calcifications (arrow) in the anterior mediastinal mass without significant enhancing solid tissue
Lipoma
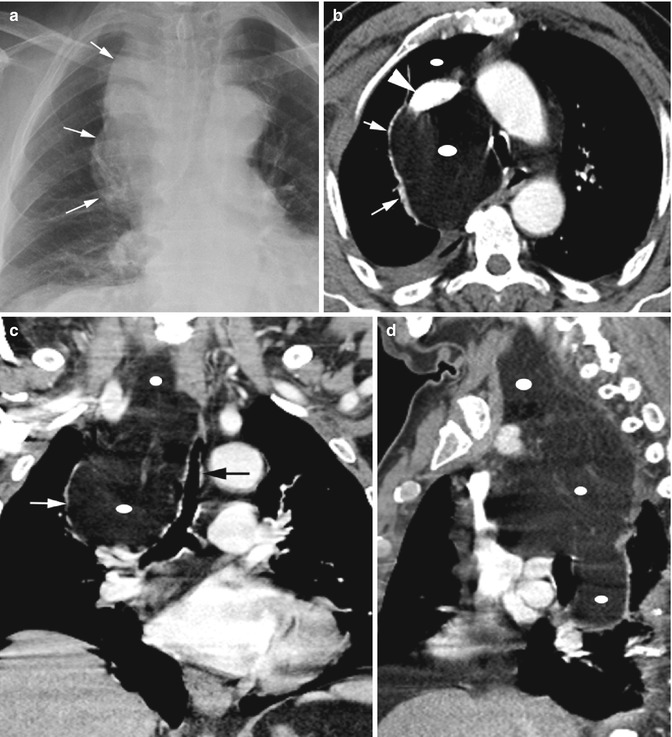
Fig. 10.16
Lipoma of the mediastinum. Chest radiograph (a) shows a large mass in the right paratracheal region (arrows) with extrinsic pressure on the trachea. (b–d) Axial CT and coronal and sagittal reformatted images show a large lipoma (ellipse) in the right side of the mediastinum extending into the neck on the medial side of the common carotid artery up to the level of the larynx. It is causing extrinsic pressure on the SVC (arrowhead) and is displacing the azygos vein (thin white arrows) and the trachea (thick black arrow)
Esophageal Lesions
Diagnosis
Foreign Body in the Esophagus
Imaging Features
1.
Metallic coin in the esophagus posterior to the trachea as seen in lateral view
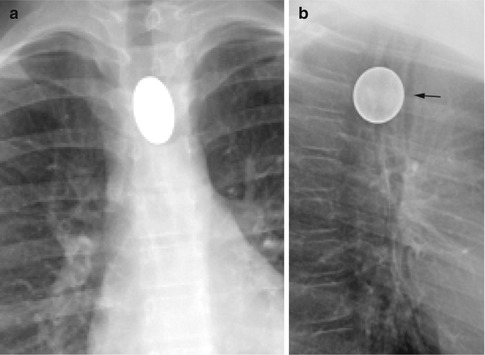
Fig. 10.17
Coin in the esophagus. (a, b) PA and lateral chest images show an esophageal coin with the tracheal air column anterior (arrow) to the coin. The rounded appearance of the coin in the lateral view is contrary to the truism
Diagnosis
Bone in the Esophagus
Imaging Features
1.
Elongated calcified density in the esophagus, behind the trachea at the thoracic inlet
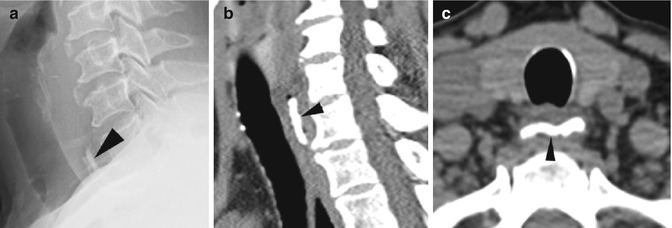
Fig. 10.18
Bone in the esophagus. (a) Lateral view of the neck shows a radio-opaque bone (arrowhead) in the esophagus at the thoracic inlet behind the trachea. (b, c) Sagittal reformatted and axial CTs confirm the radiographic findings (arrow head)
Diagnosis
Bronchoesophageal Fistula
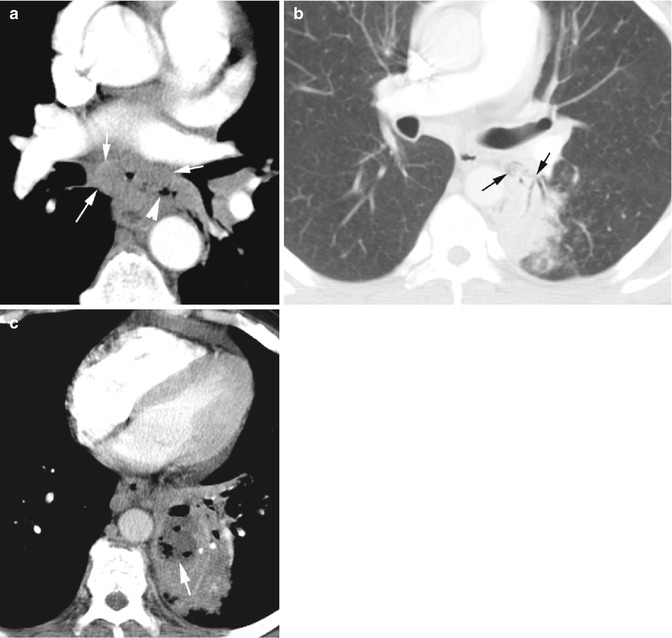
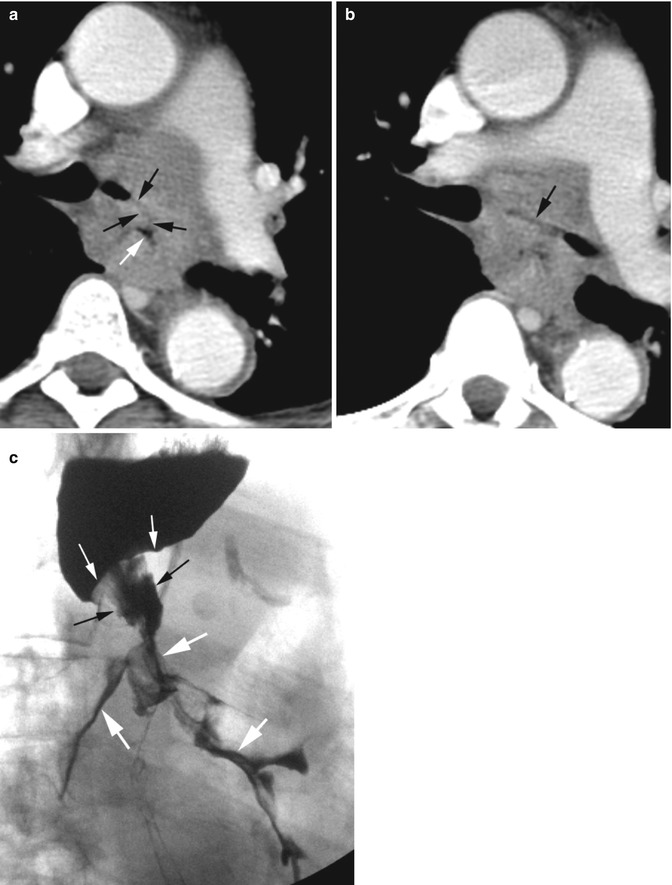
Fig. 10.19
Esophageal carcinoma with bronchoesophageal fistula and abscess formation. Axial CT (a) shows soft tissue mass (white arrows) surrounding the infra-carinal esophagus which shows perforation with gas extending outside the lumen (arrowhead). (b) Gas and fluid are seen communicating with the left lower lobe bronchus (black arrows). (c) Abscess with loculated gas and fluid collection in the consolidated lung in the left lower lobe (thick arrow)
Fig. 10.20
Esophageal carcinoma at the carina encasing the left main stem bronchus with fistulous communication. (a) Axial CT shows a faint fistulous tract (black arrows) from the esophagus (white arrow) to the trachea. (b) Axial CT at a lower plane than the fistulous tract shows narrowed fluid-filled left main stem bronchus (arrow). (c) Barium swallow study contrast in the left lower lobe bronchi (thick white arrows) from the abrupt irregular narrowed esophagus (black arrows) with shelflike transitional zone (thin white arrows)