CHAPTER 13 MRI examination of the wrist has been slower to develop than that of other joints. Similarly, wrist arthrography has not enjoyed the same popularity as that of the knee or shoulder. Nevertheless, MRI of the wrist has some definite utility. It is useful in evaluating the carpal bones for fractures and avascular necrosis (AVN). It seems to have some use for evaluating the triangular fibrocartilage (TFC) and the intercarpal ligaments.1 Thin-section (2 to 3 mm) T1- and T2-weighted images in both an axial and a coronal plane are typically used with a dedicated wrist coil or a small surface coil. Some recommend sagittal images as well. A small field of view (FOV; 5 to 8 cm) should be used for maximal resolution. Three-dimensional volumetric coronal images with thin (1 to 2 mm) slices are used in many centers to replace the T2-weighted images. These are especially useful for examining the TFC and the intercarpal ligaments.2 The normal TFC is predominantly low signal on all imaging sequences and seen to be triangular in shape, with the base attaching to the ulna and the apex attaching onto the radius (Figure 13-1). A detached or torn TFC is best seen in the coronal plane with T2 or gradient-echo sequences and is usually accompanied by joint fluid in both the distal radioulnar and the proximal carpal joints (Figure 13-2). FIGURE 13-1 The wrist has several bones that have a propensity to undergo AVN. The lunate is commonly affected and is known as Kienböck’s malacia. It is seen as uniform low signal on T1- and T2-weighted images (Figure 13-3). As is found with AVN in other joints, MRI examination can be useful in showing AVN when plain films are normal. FIGURE 13-3 The proximal pole of the scaphoid often undergoes AVN after a fracture is sustained. MRI can demonstrate the AVN earlier than plain films, allowing earlier treatment (Figure 13-4). Subtle or occult fractures of the scaphoid (or any other carpal bone) can be identified with MRI examination. MRI should be considered when clinical suspicion of a fracture is high and plain films are negative, because a missed fracture of the scaphoid can lead to AVN. We have found it cost-effective to obtain an MRI scan of the wrist to rule out a fracture in a patient with trauma, pain in the snuffbox, and a negative plain film, as opposed to casting the patient for a week and having him or her return for a follow-up x-ray examination.3 FIGURE 13-4 The intercarpal ligaments can tear and cause pain and instability in the wrist. The scapholunate ligament is the most commonly torn intercarpal ligament. It should be identified at the proximal part of the scapholunate joint in every MRI scan of the wrist unless it is torn (Figure 13-5). A torn scapholunate ligament will have linear disruption of the normal triangular or bandlike configuration (Figure 13-6). The next most common intercarpal ligament to tear is the lunatotriquetral ligament, which is found at the proximal portion of the joint. Unfortunately it is not always visualized, even with excellent images; hence, it is difficult to diagnose a torn lunatotriquetral ligament with any certainty. FIGURE 13-5
Miscellaneous magnetic resonance imaging
Wrist
Imaging techniques
Pathology
Triangular fibrocartilage
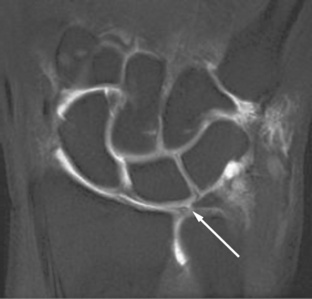
 Normal TFC. A coronal gradient-echo 3D-volume thin-section image of a normal wrist shows the TFC (arrow) with its attachment to the radius separated by a thin layer of cartilage.
Normal TFC. A coronal gradient-echo 3D-volume thin-section image of a normal wrist shows the TFC (arrow) with its attachment to the radius separated by a thin layer of cartilage.
Avascular necrosis

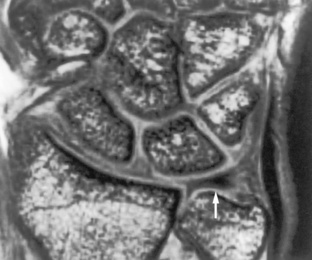
 Kienböck’s malacia. A coronal T1-weighted image shows the lunate (arrow) to be devoid of the normal high signal from fatty marrow. This is diagnostic of AVN and is called Kienböck’s malacia when it occurs in the lunate.
Kienböck’s malacia. A coronal T1-weighted image shows the lunate (arrow) to be devoid of the normal high signal from fatty marrow. This is diagnostic of AVN and is called Kienböck’s malacia when it occurs in the lunate.
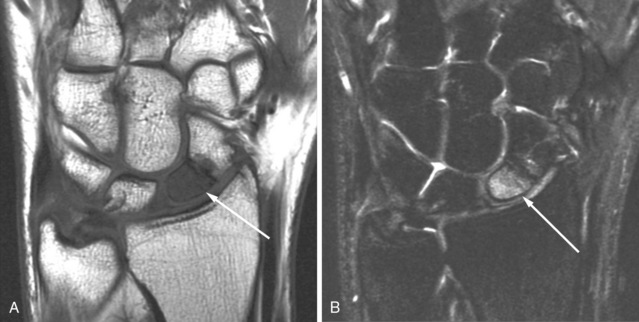
 Scaphoid AVN. Coronal images in a patient who sustained a fracture of his scaphoid several months prior shows low signal in the proximal pole on the T1-weighted images (A), which is high in signal on the T2-weighted images (B). This is worrisome but not diagnostic of AVN. If the T2-weighted images were low in signal, it would indicate AVN; however, with high T2 signal, the proximal pole might still be viable.
Scaphoid AVN. Coronal images in a patient who sustained a fracture of his scaphoid several months prior shows low signal in the proximal pole on the T1-weighted images (A), which is high in signal on the T2-weighted images (B). This is worrisome but not diagnostic of AVN. If the T2-weighted images were low in signal, it would indicate AVN; however, with high T2 signal, the proximal pole might still be viable.
Intercarpal ligaments
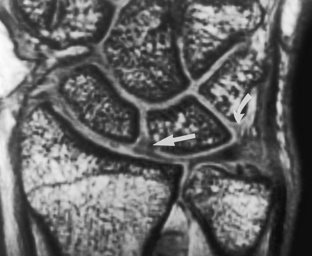
 Scapholunate ligament. A coronal 3D-volume thin-section image of a normal wrist shows the appearance of the scapholunate ligament (arrow). A normal lunotriquetral ligament (curved arrow) can also be seen, although it is not always identified.
Scapholunate ligament. A coronal 3D-volume thin-section image of a normal wrist shows the appearance of the scapholunate ligament (arrow). A normal lunotriquetral ligament (curved arrow) can also be seen, although it is not always identified.