MR imaging is ideally suited for characterization of the soft tissue, cartilaginous, and osseous structures of the pediatric ankle. An understanding of the normal MR imaging appearance associated with the dynamic skeletal maturation process will prevent overdiagnosis and unnecessary treatment. In this article, we review the normal MR imaging appearance of the growing ankle as well as several disease processes unique to the pediatric population.
Key points
- •
The MR appearance of the pediatric foot and ankle depends on the predictable pattern of chondral, osseous, and marrow maturation.
- •
An understanding of normal age-related development is essential to differentiating normal findings from common pathologies.
- •
The distal tibial and fibular physes have undulating, trilaminar appearances with consistent width until skeletal maturity; physeal widening or bridging indicates disrupted endochondral ossification.
- •
Epiphyseal and tarsal ossification centers are surrounded by secondary physes, identical to primary physes. Osteochondral abnormalities often result from injury/insult to the secondary physis.
- •
Residual hematopoietic marrow has a characteristic appearance in the foot and ankle and may persist into young adulthood.
Introduction
The MR imaging appearance of the pediatric ankle reflects the dynamic process of skeletal growth and maturation. An understanding of the normal age-related development within the chondroosseous structures is essential to an appreciation of the common pathologic conditions affecting the ankle in children. This article focuses on the MR imaging appearance of the maturing ankle and the disorders that can impact this appearance. The imaging manifestations of trauma, developmental disorders, infection, avascular necrosis, and tumors depend on the developmental maturation of the physis, epiphysis/apophysis, and marrow.
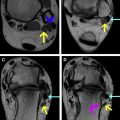
In the neonate, the epiphyses at the distal ends of the tibia and fibula are composed entirely of hyaline cartilage, and the physes separating the epiphyses from the metaphyses are transversely oriented. The ultimate shape and growth of the ends of these long bones depends on a balance between endochondral ossification and intramembranous ossification. Endochondral ossification is the highly organized process converting cartilage to bone. The primary physis provides for linear growth of the long bones and centrifugal growth of the tarsal bones, whereas the secondary physis that surrounds the secondary center of ossification is responsible for spherical growth of the epiphyses. The periosteum contributes to transverse growth (diameter increase) of the long bones through intramembranous ossification with direct mineralization of the vascular connective tissue without a cartilaginous mold. This dynamic ossification process dictates the age-related appearance of the ankle on MR images. In the newborn period, epiphyseal cartilage is homogeneously intermediate signal intensity on T1-weighted images (T1WI) and low signal intensity on water-sensitive sequences. The high water concentration of marrow in the newborn period leads to homogeneous low signal intensity on T1WI and high signal intensity on water-sensitive sequences. As the secondary ossification centers appear and the marrow converts from hematopoietic to fatty, the adult MR imaging features develop with a predictable pattern ( Fig. 1 ).

The vascularity of the growing bones predisposes to pathology and its associated appearance. Transphyseal vascular canals in infants and toddlers allow infection and tumor to pass between the metaphysis and epiphysis. These channels disappear by 18 months of age and do not normally recur until skeletal maturity. If these transphyseal vascular communications are reestablished owing to trauma, endochondral ossification along the vessels may ensue leading to physeal bone bridge formation. Embryologic vascular channels may persist within the epiphyses and epiphyseal equivalents and should not be confused for infection or tumor. This is most commonly seen in the mid portion of the calcaneus where vascular remnants near the insertion of the cervical and interosseous ligaments can create a moderately sized pseudolesion ( Fig. 2 ). These vascular remnants are more prevalent on MR imaging studies of children, but are also seen in adults. Table 1 summarizes several normal developmental features that may be confused for pathology.

| Normal Development | Distinguishing Feature(s) | Pathologic Mimic |
|---|---|---|
| Calcaneal vascular remnant: persistent embryologic vascular channels | Characteristic location in the mid portion of the calcaneus, extending from the sinus tarsi | Tumor or infection |
| Kump’s bump or Poland’s hump: Site of initial distal tibial physeal closure | Characteristic location in the anteromedial distal tibial physis | Fracture with osseous bridging of physis |
| Focal periphyseal edema: diminished bone flexibility at the site of transphyseal osseous fusion | Centered in the closing physis of adolescents | Physeal stress injury or infection |
| Calcaneal apophyseal fragmentation: normal developmental ossification | Absence of marrow edema or surrounding soft tissue edema, especially at the Achilles tendon insertion | Sever’s apophysitis |
| Epiphyseal ossification center irregularity, especially of the tarsal bones and malleoli: normal ossification center development | Absence of subjacent marrow edema. Intact adjacent trilaminar physis of the ossification center and articular cartilage | Osteochondritis dissecans or malleolar fracture. |
| Normal residual hematopoietic marrow | T1 signal greater than that of the adjacent muscle. Characteristic speckled appearance in the tarsal bones and geometric shape tethered to physis in long bones. | Stress-related edema. Perivascular foci of red marrow often magnified by osteoporosis from disuse |
Introduction
The MR imaging appearance of the pediatric ankle reflects the dynamic process of skeletal growth and maturation. An understanding of the normal age-related development within the chondroosseous structures is essential to an appreciation of the common pathologic conditions affecting the ankle in children. This article focuses on the MR imaging appearance of the maturing ankle and the disorders that can impact this appearance. The imaging manifestations of trauma, developmental disorders, infection, avascular necrosis, and tumors depend on the developmental maturation of the physis, epiphysis/apophysis, and marrow.
In the neonate, the epiphyses at the distal ends of the tibia and fibula are composed entirely of hyaline cartilage, and the physes separating the epiphyses from the metaphyses are transversely oriented. The ultimate shape and growth of the ends of these long bones depends on a balance between endochondral ossification and intramembranous ossification. Endochondral ossification is the highly organized process converting cartilage to bone. The primary physis provides for linear growth of the long bones and centrifugal growth of the tarsal bones, whereas the secondary physis that surrounds the secondary center of ossification is responsible for spherical growth of the epiphyses. The periosteum contributes to transverse growth (diameter increase) of the long bones through intramembranous ossification with direct mineralization of the vascular connective tissue without a cartilaginous mold. This dynamic ossification process dictates the age-related appearance of the ankle on MR images. In the newborn period, epiphyseal cartilage is homogeneously intermediate signal intensity on T1-weighted images (T1WI) and low signal intensity on water-sensitive sequences. The high water concentration of marrow in the newborn period leads to homogeneous low signal intensity on T1WI and high signal intensity on water-sensitive sequences. As the secondary ossification centers appear and the marrow converts from hematopoietic to fatty, the adult MR imaging features develop with a predictable pattern ( Fig. 1 ).
The vascularity of the growing bones predisposes to pathology and its associated appearance. Transphyseal vascular canals in infants and toddlers allow infection and tumor to pass between the metaphysis and epiphysis. These channels disappear by 18 months of age and do not normally recur until skeletal maturity. If these transphyseal vascular communications are reestablished owing to trauma, endochondral ossification along the vessels may ensue leading to physeal bone bridge formation. Embryologic vascular channels may persist within the epiphyses and epiphyseal equivalents and should not be confused for infection or tumor. This is most commonly seen in the mid portion of the calcaneus where vascular remnants near the insertion of the cervical and interosseous ligaments can create a moderately sized pseudolesion ( Fig. 2 ). These vascular remnants are more prevalent on MR imaging studies of children, but are also seen in adults. Table 1 summarizes several normal developmental features that may be confused for pathology.
| Normal Development | Distinguishing Feature(s) | Pathologic Mimic |
|---|---|---|
| Calcaneal vascular remnant: persistent embryologic vascular channels | Characteristic location in the mid portion of the calcaneus, extending from the sinus tarsi | Tumor or infection |
| Kump’s bump or Poland’s hump: Site of initial distal tibial physeal closure | Characteristic location in the anteromedial distal tibial physis | Fracture with osseous bridging of physis |
| Focal periphyseal edema: diminished bone flexibility at the site of transphyseal osseous fusion | Centered in the closing physis of adolescents | Physeal stress injury or infection |
| Calcaneal apophyseal fragmentation: normal developmental ossification | Absence of marrow edema or surrounding soft tissue edema, especially at the Achilles tendon insertion | Sever’s apophysitis |
| Epiphyseal ossification center irregularity, especially of the tarsal bones and malleoli: normal ossification center development | Absence of subjacent marrow edema. Intact adjacent trilaminar physis of the ossification center and articular cartilage | Osteochondritis dissecans or malleolar fracture. |
| Normal residual hematopoietic marrow | T1 signal greater than that of the adjacent muscle. Characteristic speckled appearance in the tarsal bones and geometric shape tethered to physis in long bones. | Stress-related edema. Perivascular foci of red marrow often magnified by osteoporosis from disuse |
Physeal development
The distal tibial and fibular physes are highly organized cartilaginous structures responsible for linear growth of the ankle. T2-weighted fat-suppressed MR images are best suited for evaluation of the physis, which has a trilaminar appearance, with high signal intensity in the physeal resting and hypertrophic zones adjacent to the epiphysis, low signal intensity in the zone of provisional calcification, and high signal intensity in the metaphyseal vascular primary spongiosa (see Fig. 1 ). Physeal cartilage has a higher signal intensity than the adjacent epiphyseal cartilage on long repetition time sequences owing to the greater amount of free water in the physeal hyaline cartilage. By 2 years of age, the distal tibial physis is normally undulating with a focal anteromedial upward deviation often called Kump’s bump or Poland’s hump. This represents the site of initial physiologic physeal closure, which is completed in girls from 12 to 15 years and boys from 15 to 18 years ( Fig. 3 ). This asymmetric early physeal fusion tethers the growth plate and predisposes to Tillaux (Salter Harris type III) and triplane physeal fractures in this age group. Distal tibial physeal fractures have a high rate of growth arrest because the undulating physis predisposes to the creation of transphyseal vascular connections and subsequent physeal bone bridge formation at the fracture site. Large bone bridges lead to limb length discrepancy, whereas small, eccentric bridges lead to angular deformity. Growth recovery lines tethered to the physis, best seen on T1WI, indicate asymmetric physeal growth ( Fig. 4 ). The distal fibular physis is highly undulating, especially laterally where the peripheral margins can be spiculated and should not be mistaken for fracture.
The distal tibiofibular physeal relationship is dynamic early in growth. In infancy, the distal fibular physis is at the level of the midpoint of the tibial epiphysis. By 5 years of age, the distal fibular physis has migrated to the level of the distal tibial articular surface. Disruption of this relationship indicates growth disturbance. Additionally, the physis should be uniform in thickness throughout growth up until skeletal maturity. Physeal widening, either diffuse or focal owing to unossiffied physeal cartilage extending into the metaphysis, indicates physeal injury and disruption of endochondral ossification ( Fig. 5 ). This growth disturbance is typically the result of chronic overuse stress in young athletes.