Accessory muscles around the ankle are commonly encountered as incidental findings on cross-sectional imaging. Mostly asymptomatic, accessory muscles sometimes mimic mass lesions. They have been implicated as the cause of tarsal tunnel syndrome, impingement of surrounding structures, and chronic pain. Distinguishing these muscles can be challenging, because some travel along a similar path. This article describes these accessory muscles in detail, including their relationships to the aponeurosis of the lower leg. An imaging algorithm is proposed to aid in identification of these muscles, providing a valuable tool in diagnostic accuracy and subsequent patient management.
Key points
- •
Accessory muscles are commonly presented as incidental findings on cross-sectional imaging.
- •
Although most often asymptomatic, accessory muscles sometimes mimic mass lesions, and have been implicated as the cause of tarsal tunnel syndrome, impingement of surrounding structures, and pain related to muscle ischemia. Unless specifically injured, accessory muscles appear isointense to other muscles on all imaging sequences.
- •
Based on the location of the accessory muscles, including their origins, insertions, and relationships to the aponeurosis of the lower leg, an imaging algorithm is proposed to aid in their identification.
Introduction
Anatomic variations of muscles around the ankle consist predominantly of extra or accessory muscles. Generally asymptomatic, these supernumerary muscles are discovered incidentally on imaging studies. Accurate diagnosis of the infrequent symptomatic cases, presenting as mass lesions, tarsal tunnel syndromes, chronic ankle pain, or impingement, is important for management. However, distinguishing between these muscles can be challenging, because some travel along a similar path, and others have either similar origins or similar insertions. This article reviews each accessory muscle in detail, including those located lateral and posteromedial to the ankle. Each muscle’s origin, insertion, imaging features, and clinical presentations, along with its relationship with the aponeurosis of the lower leg, are described ( Table 1 ). In an effort to improve diagnostic accuracy, an imaging algorithm that can be readily applied in daily practice is proposed.
| Origin | Course | Insertion | Alternative Name | Relative to Deep Aponeurosis | Notes | |
|---|---|---|---|---|---|---|
| Lateral Accessory Muscle | ||||||
| PQ | Alternative Name of PQ Based on Insertion | The insertion site is highly variable, which gives rise to subtypes and confusing terminology | ||||
| Retrotrochlear eminence (most common insertion) Cuboid Peroneus longus | Peroneocalcaneus externum | |||||
| Posterior surface of the fibula or peroneus longus or peroneus brevis | Travels medial and posterior to the peroneal tendons | Peroneocuboideus | ||||
| Peroneoperoneolongus | ||||||
| Inferior retinaculum | ||||||
| Posteromedial Accessory Muscles | ||||||
| Accessory soleus | Fibula, or soleal line of the tibia, or the anterior surface of the soleus muscle | Descends posterior to the neurovascular bundle | Upper or medial, calcaneal surface | Superficial | ||
| FDAL | Variable origin, can arise from any structures of the posterior compartment | Descends with the posterior tibial neurovascular bundle in the tarsal tunnel | Quadratus plantae, or the FDL before its division | Long accessory of the quadratus plantae Long accessory of the long flexors Accessorius of the accessorius of Turner Second accessorius of Humphrey | Deep | Compare with other accessory muscles in or near the tarsal tunnel, such as the TCI or PCI; the FDAL does not insert onto the calcaneus |
| PCI | Lower third of the fibula | Travels parallel to but remains lateral to the FHL | Base of the sustentaculum | Deep | Not directly related to the neurovascular bundle, because it travels lateral to the FHL | |
| TCI | Medial crest of the tibia | Travels posterior to the FHL, within the tarsal tunnel and superficial to the neurovascular bundle | Medial calcaneus | Deep | Has features of both the FDAL and the accessory soleus | |
Introduction
Anatomic variations of muscles around the ankle consist predominantly of extra or accessory muscles. Generally asymptomatic, these supernumerary muscles are discovered incidentally on imaging studies. Accurate diagnosis of the infrequent symptomatic cases, presenting as mass lesions, tarsal tunnel syndromes, chronic ankle pain, or impingement, is important for management. However, distinguishing between these muscles can be challenging, because some travel along a similar path, and others have either similar origins or similar insertions. This article reviews each accessory muscle in detail, including those located lateral and posteromedial to the ankle. Each muscle’s origin, insertion, imaging features, and clinical presentations, along with its relationship with the aponeurosis of the lower leg, are described ( Table 1 ). In an effort to improve diagnostic accuracy, an imaging algorithm that can be readily applied in daily practice is proposed.
| Origin | Course | Insertion | Alternative Name | Relative to Deep Aponeurosis | Notes | |
|---|---|---|---|---|---|---|
| Lateral Accessory Muscle | ||||||
| PQ | Alternative Name of PQ Based on Insertion | The insertion site is highly variable, which gives rise to subtypes and confusing terminology | ||||
| Retrotrochlear eminence (most common insertion) Cuboid Peroneus longus | Peroneocalcaneus externum | |||||
| Posterior surface of the fibula or peroneus longus or peroneus brevis | Travels medial and posterior to the peroneal tendons | Peroneocuboideus | ||||
| Peroneoperoneolongus | ||||||
| Inferior retinaculum | ||||||
| Posteromedial Accessory Muscles | ||||||
| Accessory soleus | Fibula, or soleal line of the tibia, or the anterior surface of the soleus muscle | Descends posterior to the neurovascular bundle | Upper or medial, calcaneal surface | Superficial | ||
| FDAL | Variable origin, can arise from any structures of the posterior compartment | Descends with the posterior tibial neurovascular bundle in the tarsal tunnel | Quadratus plantae, or the FDL before its division | Long accessory of the quadratus plantae Long accessory of the long flexors Accessorius of the accessorius of Turner Second accessorius of Humphrey | Deep | Compare with other accessory muscles in or near the tarsal tunnel, such as the TCI or PCI; the FDAL does not insert onto the calcaneus |
| PCI | Lower third of the fibula | Travels parallel to but remains lateral to the FHL | Base of the sustentaculum | Deep | Not directly related to the neurovascular bundle, because it travels lateral to the FHL | |
| TCI | Medial crest of the tibia | Travels posterior to the FHL, within the tarsal tunnel and superficial to the neurovascular bundle | Medial calcaneus | Deep | Has features of both the FDAL and the accessory soleus | |
Imaging of accessory muscles
Although the accessory muscles of the ankle can be detected on all cross-sectional imaging modalities, most published reports are of magnetic resonance (MR) imaging studies because of its superior soft tissue contrast. However, MR imaging does have limitations. First, the origins of these muscles may not be included in the field of view of a routine ankle examination. Second, if insertions are small, they can be difficult to separate from surrounding soft tissues. Lateral radiography captures only the accessory soleus and is therefore of limited use.
Accessory muscles in the lateral ankle
Peroneus Quartus
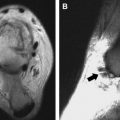
The peroneus quartus (PQ) ( Fig. 1 ) refers to the fourth peroneal muscle, after peroneus longus, peroneus brevis, and peroneus tertius. It represents a group of accessory peroneal muscles found only in humans. Its absence in other species and its function in stabilizing hind foot pronation led Hecker to postulate that these muscles are evolutionary developments to accommodate the bipedal posture.

The reported prevalence of the PQ ranges from 5.2% to 22%. A systematic review pooling 46 studies reported 16% prevalence. The most common subtype is the peroneocalcaneus externum, found in 79% and 91% of all PQ.
Origin
The origin is variable and includes the posterior surface of the fibula or an origin from the peroneus longus or peroneus brevis muscle. Origin from the peroneus brevis origin is the most common based on both cadaveric studies and imaging.
Insertion
The insertion site is highly variable, which gives rise to subtypes and confusing terminology ( Fig. 2 ). Hecker’s classification, based on the various insertions, is listed in Table 2 .
| Insertion Site | Alternative Name of PQ Based on Insertion |
|---|---|
| Retrotrochlear eminence a | Peroneocalcaneus externum |
| Cuboid | Peroneocuboideus |
| Peroneus longus | Peroneoperoneolongus |
| Inferior retinaculum |
The most common insertion of the PQ is at the retrotrochlear eminence, one of 2 bony protuberances arising from the lateral cortex of the calcaneus (see Fig. 1 ). The retrotrochlear eminence lies posterior to the peroneal tubercle, which separates the 2 peroneal tendons.
Imaging Features
The tendon is described mostly in MR and infrequently in ultrasonography (US) studies. The accessory muscle is seen as a separate structure traveling medial and posterior to the peroneal tendons (see Fig. 2 ). Its origin may be difficult to separate from the peroneal muscles. It becomes tendinous with variable insertions (see Fig. 2 and Table 2 ).
Clinical Features
Although generally asymptomatic, the PQ muscles may contribute to crowding in the peroneal tunnel ( Fig. 3 ), thereby predisposing patients to peroneal tendinopathy, peroneal brevis dislocation, synovitis, pain, and snapping. The use of PQ for repair of the superior peroneal retinaculum has also been reported.