CHAPTER 4 MRI of the Lower Extremities
MRI of the lower extremities—considerations
Scan Considerations
• Extremities should be scanned in the anatomical position when possible. Consider the patients tolerance for pain; a neutral position may be necessary.
• When scanning long bones, it may be difficult to fit the anatomy into a single coil. Repositioning the patient may be required.
• Place a vitamin E, capsule or MRI-compatible market at the area of pain or interest.
• Refer to all safety-related parameters.
• As the SAR (specific absorption rate) increases, the patient’s body temperature will also increase. SAR elevation can be compensated for by increasing the TR slightly. If this is not done correctly at 3T, the SAR will increase and scanner will stop as a patient safety precaution. All 3T systems have SAR monitors that should be referenced while scanning. This is not an issue at 1.5T.
• Contrast is often used for osteomyelitis, tumor, or infection.
• MR arthrogram is performed to best demonstrate labral and intra-articular pathology of the hip. A mixture of gadolinium and iodinated contrast is injected into the bursa in a fluoroscopy suite before the MRI is performed. Indirect arthrography can be performed after injecting gadolinium into a vein and waiting a period of time while exercising the affected joint.
• Orthopedic hardware can cause distortion and metallic artifacts in the image. To help compensate, the bandwidth should be increased, the ETL can be increased, and the NEX (number of excitations) can be increased. These options will help but not eliminate these artifacts.
Coils
• Multi-channel body-specific coils are used when available. Any coil that covers the anatomy may be used, i.e., the cardiac coil may be used to scan the hip.
• All multi-channel coils produce excessive single adjacent to the coil. This can be compensated for by using vendor-specific options to provide uniform single intensity.
Pulse Sequences
• T1 is used to best identify anatomic structures, whereas T2 fat saturation (FS) and or STIR (short T1 inversion recovery) provides detailed evidence of pathology.
• On T1 sequences, bones should appear bright or hyperintense because fat in the bone has a short relaxation time. If not, a disease process can be present. On T1 Sequences, fluid will appear dark or hyperintense because water has a long T1 relaxation time.
• On T2 sequences, fluid produces bright or hyperintense signal as a result of long T2 relaxation. T2 imaging uses FS or STIR to eliminate the fat and enhance abnormal fluid or pathology in bone.
• T1 FS is used post routine arthrogram to best visualize the contrast in the joints. T2 FS may also be added when indicated.
• T1 and/or T2 CUBE can be used to obtain high-resolution submillimeter images of the ankle.
Options
• FS options and terminology are vendor-specific. For GE system, use “fat classic” for FS with enhanced anatomical detail.
• IDEAL (GE) is a fat/water separation technique (previously called 3-point Dixon technique). This technique eliminates fat and water and provides an in and out of phase image, all in one acquisition. IDEAL can be used with T1, T2, and SPGR pulse sequences.
• Superior and inferior saturation bands help to compensate for vascular pulsation, whereas left or right saturation bands can help compensate for breathing or cardiac motion. Saturation bands can be used on all pulse sequences.
• Flow compensation (FC) or gradient nulling should be used on T2 images to help compensate for vascular motion.
MRI of the hips
Acquire three-plane pilot per site specifications.

COIL: Multi-channel vendor-specific torso coil or cardiac coil
POSITION: Supine, feet first, legs flat and extended with feet inverted
IMMOBILIZATION: Place cushion between the ankles to support inversion of feet. Secure feet with tape.
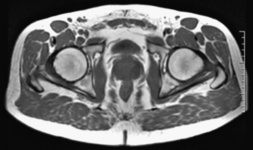
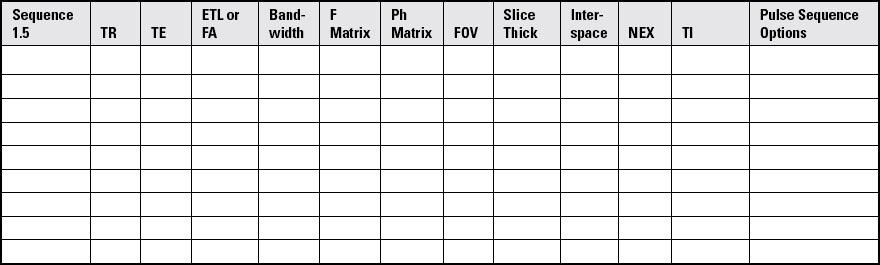
Acquisition of Axial Image of the Hips
Hips are scanned bilaterally in the axial and coronal plane; sagittal sequences are unilateral.
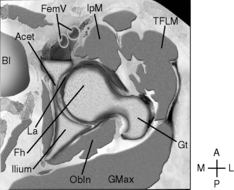
SLICE ACQUISITION: Superior to inferior
SLICE ALIGNMENT: Parallel to the femoral heads
ANATOMIC COVERAGE: Iliac fossa to proximal femur, including the lesser trochanter
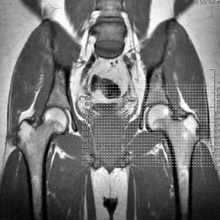
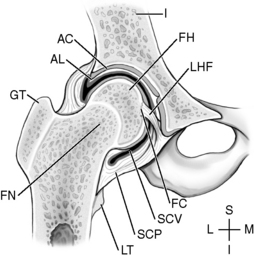
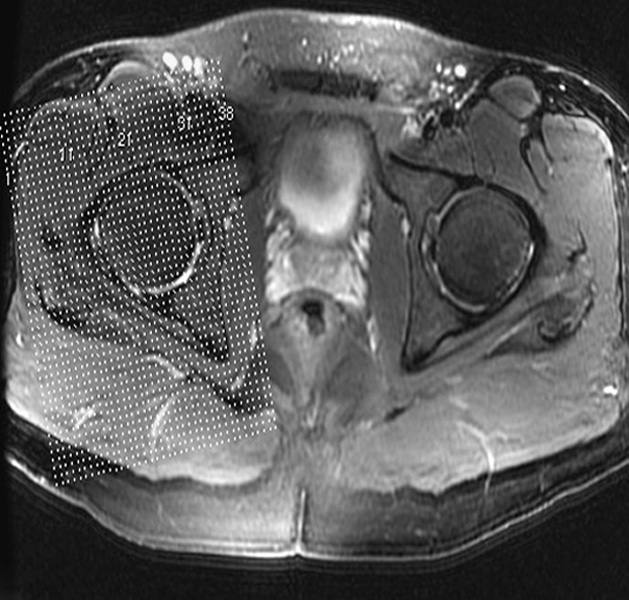
Acquisition of Coronal Image of the Hips
Hips are scanned bilaterally in the axial and coronal plane, and sagittal sequences are unilateral.

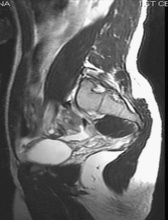
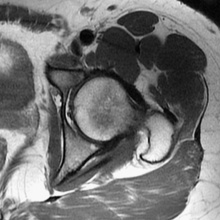
Acquisition of Sagittal Image of the Hips
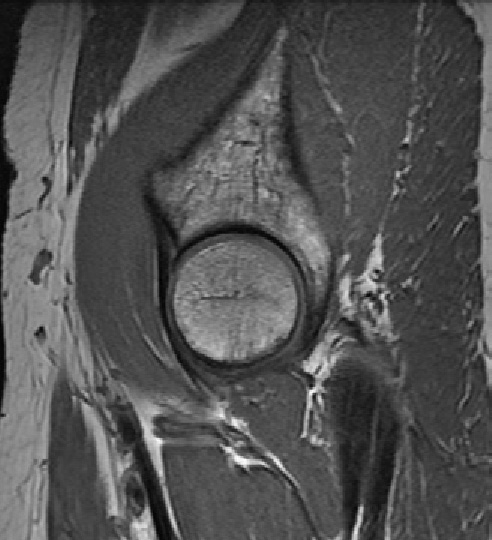
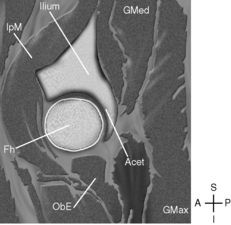
SLICE ACQUISITION: Lateral to medial
SLICE ALIGNMENT: Parallel to the labrum of the acetabulum
ANATOMIC COVERAGE: Greater trochanter to the superior pubic ramus
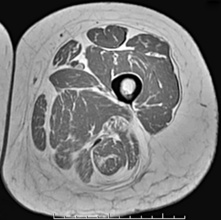
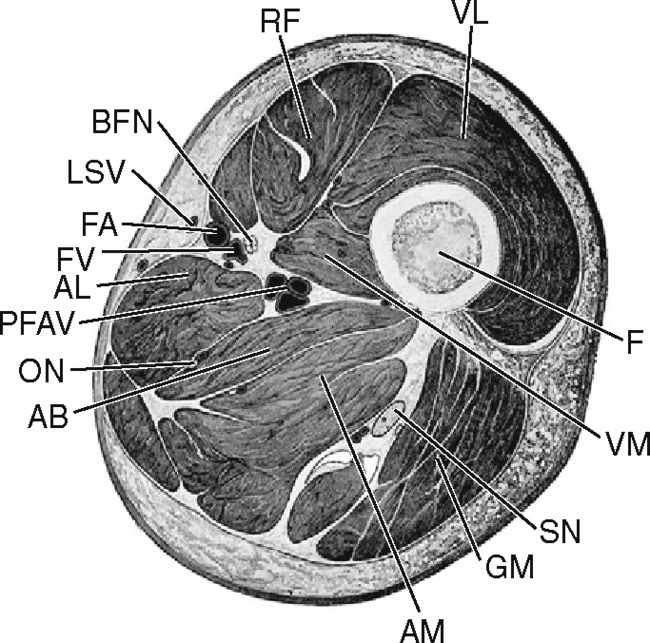
MRI of the femur
Acquire three-plane pilot per site specifications.

COIL: Vendor-specific eight-channel torso coil or cardiac coil.
POSITION: Supine, feet first, legs flat and extended with feet inverted.
LANDMARK: Midshaft of the femur
IMMOBILIZATION: Place a cushion between the ankles to support inversion of feet. Secure patient’s feet with tape.
Use long-bone protocol. FOV is determined by the anatomy to be covered.
If off center, the FOV diminishes adequate fat saturation; STIR should be performed.
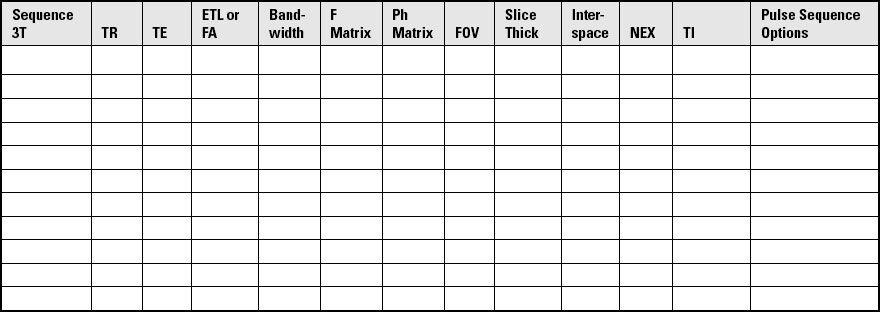
Acquisition of Coronal Image of the Femur



SLICE ACQUISITION: Anterior to posterior
SLICE ALIGNMENT: Parallel to the shaft of the femur
ANATOMICAL COVERAGE: Head of femur to proximal tibia; include musculature of the thigh.