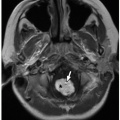
 FIGURE 22.1 Radiography. Five-year-old girl who presented to the emergency room with knee pain and limping. A: Initial frontal radiograph shows a subtle lucency (arrow) in the lateral epiphysis of the distal femur. B: Follow-up MRI examination performed 10 days after onset of symptoms shows progression of the epiphyseal abnormality, which now abuts the physis and presents with further bony destruction. Increased signal consistent with bone marrow edema is seen on the coronal short tau inversion recovery (STIR) image (B), which corresponds to low signal on coronal T1-weighted MR image (C) in the epiphysis surrounding the focal bone abscess. Axial STIR (D) and axial post-contrast fat-suppressed T1-weighted (E) MR images show debris levels (arrow) within the intraosseous abscess, which does not enhance centrally. Peripheral rim enhancement is noted in the abscess (E). |
 FIGURE 22.2 Radiographic sequelae of osteomyelitis. Pathologic fracture through the proximal humerus in a preschool child with sickle cell disease and features of chronic osteomyelitis include diffuse cortical thickening of the diaphysis and bone expansion. |
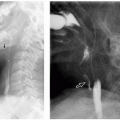
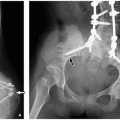
 FIGURE 22.3 Radiographic sequelae of osteomyelitis. One-month-old infant boy with a focal lucency (arrow) in the left proximal femoral metaphysis that is subluxed superolaterally (A). Four years later, follow-up radiograph (B) demonstrates progression with hip dislocation, complete destruction of the epiphysis, and remodeling of the metaphysis. |
 FIGURE 22.4 Radiographic sequelae of osteomyelitis. Chronic sequela of meningococcemia in infancy. Frontal radiograph of both knees obtained 3 years after the meningococcemia episode (A) shows multiple metaphyseal and epiphyseal lucencies with irregularity of the growth plates. Scanogram of lower extremities obtained a decade later (B) shows premature physeal fusion with resultant length discrepancy. Note the fibular bowing (arrow) due to tethering from the severely shortened tibia. |
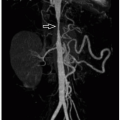
 FIGURE 22.5 Ultrasound. Normal frontal radiograph of right tibia and fibula in a child with clinical suspicion for osteomyelitis (A). Ultrasound performed on the following day (B) shows a large subperiosteal abscess (arrow) along the proximal fibular metadiaphysis. Corresponding color Doppler ultrasound imaging (C) shows hyperemia in the adjacent soft tissues. The normal contralateral left side is included for comparison. |
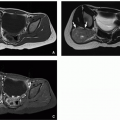
 FIGURE 22.6 Ultrasound and nuclear medicine. Infant boy who presented with fever, irritability, and lack of mobility of the left lower extremity. Longitudinal grayscale ultrasound (A) shows large effusion (calipers) in the left hip. Ultrasound image of the contralateral asymptomatic hip (B) is shown for comparison. Bone scan performed on the same day of the ultrasound scan (C) demonstrates increased uptake in the proximal femur and left hip joint (arrow) suggesting septic arthritis. Aspiration of pus from the hip joint and culture of the material confirmed the diagnosis. |
from reactive inflammation as well as its difficulty with evaluating regions with metallic implants.
of osteomyelitis depends on the patient’s age, affecting most commonly the epiphysis in neonates and infants and the metaphysis in older children. Hematogenous infection typically begins in the metaphysis secondary to its abundant blood supply. Patterns of spread of infection change with varying age groups because of differences in the microanatomy of the vascular supply with growth (Fig. 22.9).22,23
 |
 FIGURE 22.7 MR imaging. Preadolescent girl with a focal metaphyseal lucency (arrow) in the distal radius on the frontal radiograph of wrist (A). Hyperintense signal on the coronal fat-suppressed T2-weighted MR image (B) and hypointense signal on the coronal T1-weighted MR image (C) highlight the extensive bone marrow edema in the metaphysis and epiphysis of the distal radius. Epiphyseal involvement is related to the metaphyseal abscess, which is also seen penetrating the physis. Sagittal post-contrast fat-suppressed T2-weighted MR image (D) shows diffuse enhancement in the bone marrow and rim enhancement in the transphyseal abscess (asterisk) with associated pyomyositis. |
 FIGURE 22.8 Nuclear medicine. Lateral radiographic view of the foot (A) demonstrates a subtle lucency (arrow) in the calcaneus in a child who presented with pain and swelling. Flow (B) and blood pool (C) images from the technetium 99-MDP bone scan confirm increased uptake (arrow) in the body of the calcaneus consistent with osteomyelitis. |
 FIGURE 22.9 Modes of spread of infection. A: In an infant: Infection originating in the highly vascularized metaphysis can extend into the epiphysis via patent transphyseal vessels. If it spreads into the joint, it results in septic arthritis. If it extends underneath the periosteum, it results in a subperiosteal abscess (collection). B: In an older child: Subacute osteomyelitis demonstrates a Brodie abscess surrounded by a local involucrum. In chronic osteomyelitis, spread of infection into the soft tissues following cortical damage can occur through a cloaca. |
 FIGURE 22.10 Modes of spread of infection. A: Infant blood supply demonstrates continuity of the metaphyseal and epiphyseal vasculature through the presence of transphyseal vessels, allowing a pathway for spread of infection. B: In the preschool child and adolescent, the transphyseal vessels are no longer patent; thus, the physis acts as a barrier to the spread of infection into the epiphysis. |
can be an initial sign of osteomyelitis, appears hypointense on T1-weighted MR images and hyperintense on T2-weighted MR images. With the administration of contrast, infected bone marrow typically enhances.16 MRI may also demonstrate regional periosteal reaction, which is caused by disrupted vascular connections that elevate the periosteum and cause new layers of periosteum (involucrum) to form.24 Spread of infection with involvement of soft tissues is manifested as increased signal intensity on T2-weighted MR images. When an abscess forms within the bone, the marrow signal intensity becomes heterogeneous, and with contrast administration, the rim of the abscess can enhance (Fig. 22.7).
TABLE 22.1 Osteomyelitis: Definitions | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
T2-weighted MR images. Surrounding the cavity is a layer of highly vascularized granulation tissue that appears isointense on T1-weighted and hyperintense on T2-weighted MR images (Fig. 22.12). This layer is best visualized on contrast-enhanced MR images because the halo enhancement corresponds to granulation tissue. Next is a fibrous layer that demonstrates low signal intensity on all MR sequences. The outer halo is composed of a peripheral rim of endosteal reaction and sclerosis that has low signal on T1-weighted and T2-weighted MR images.25 The halo enhancement on postcontrast MR images corresponds to granulation tissue. The bone marrow edema that usually surrounds the abscess
appears hypointense on T1-weighted and hyperintense on T2-weighted MR images.10,26 Brodie abscess is managed with curettage and often lengthy antibiotic treatment.27
 FIGURE 22.11 Brodie abscess. Frontal radiograph (A) of the tibia and fibula of an 8-year-old boy with a Brodie abscess shows a lytic tibial diaphyseal lesion (arrow) with associated periosteal reaction best seen on the axial CT image (B). (Continued) |
 FIGURE 22.11 (Continued) Corresponding histologic slides show pus surrounding resorbing scalloped necrotic bone (C, hematoxylin and eosin, original magnification, 600×), and clusters of gram-positive cocci (arrows) seen within the purulent material (D, Brown-Brenn stain, original magnification, 600×). This infection was subacute, having been partially treated by the parents with leftover antibiotics from their medicine cabinet before seeking medical attention. |
 FIGURE 22.12 Brodie abscess. Frontal radiograph of the left femur (A) shows a geographic lytic lesion (arrow) with sclerotic borders in the distal metaphysis. Sagittal proton density-weighted MR image of the corresponding knee (B) demonstrates the typical target appearance of a Brodie abscess (asterisk) with a hypointnse center (intraosseous abscess), a hyperintense inner ring of vascular granulation tissue (arrow) and an outer ring of low signal fibrotic tissue and sclerosis. |
 FIGURE 22.13 Features of chronic osteomyelitis. Frontal radiograph of the tibia and fibula (A) shows diffuse sclerosis, remodeling, and periosteal reaction extensively involving mainly the left tibia (arrows) of an 8-month-old infant boy representing chronic osteomyelitis. Frontal radiograph of the region of interest obtained 4 years later (B) demonstrates multifocal bone bridging resulting in overall shortening of the left tibia (arrow), marked length discrepancy, and varus alignment, as complications. |
T1- and T2-weighted MR images, with areas of increased and decreased signal intensity. Gradient-echo MR sequences can be helpful for delineation of sequestra, periosteal reaction, and involucrum because susceptibility artifacts from mineralization are exaggerated. Areas of chronic fibrosis or dead bone (including sequestrum) have low signal intensity on both T1- and T2-weighted MR images, which do not enhance with contrast. A sequestrum may be surrounded by tissue that has high-signal intensity on T1- and T2-weighted MR image and enhances with contrast (Fig. 22.14). An involucrum appears as cortical thickening with healing (Table 22.1). If the infection persists, a sinus tract or cloaca can drain pus into the adjacent soft tissues (Fig. 22.15).
 FIGURE 22.14 Features of chronic osteomyelitis. Frontal radiograph of the distal humerus of a 12-year-old boy who had undergone pinning of a supracondylar fracture 2 years previously (A) shows sclerosis, cortical thickening, and cloaca (arrow). Coronal fat-suppressed T2-weighted MR image (B) demonstrates an intraosseous abscess with a cloaca (arrow) extending superolaterally into a soft tissue abscess. (Continued) |
 FIGURE 22.14 (Continued) A low-signal sequestrum (arrow) is seen centrally in the hyperintense osseous abscess on the axial fat-suppressed T2-weighted MR image (C). Axial T1-weighted MR image (D) depicts the cloaca (arrow) along the anterior cortex. Axial post-contrast fat-suppressed T1-weighted MR image (E) shows the path of the soft tissue component of the abscess (arrowheads) tracking through the anterior cortex superficially (arrow) dissecting into the subcutaneous soft tissues. |
Bone marrow edema with or without associated enhancement.
Focal cortical destruction and associated periosteal elevation.
Associated intraosseous or juxtacortical soft tissue abscesses or edema.
Cloaca (bone marrow to periosteum) or sinus tract formation.
Sequestrum or involucrum formation.
related to primary tumors of bone is typically substantially less compared with mass-like edema related to granulation tissue from osteomyelitis.
 FIGURE 22.15 Features of chronic osteomyelitis. Sagittal T1-weighted (A) and inversion recovery (B) MR images of the ankle of a 10-year-old boy show a sinus tract, which is hypo-/isointense on T1-weighted MR image and hyperintense on T2-weighted MR image with a low signal sclerotic border. It extends from the distal tibial metaphysis into the epiphysis and through the anterior cortex into the soft tissues (arrows) with an associated soft tissue collection (arrowheads). |
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


