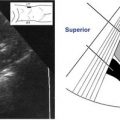
2. As illustrated on the facing page, rotate the transducer 90 degrees into the longitudinal plane to image the full length of the biceps tendon. The image demonstrates the tendon anterior to the humeral shaft and posterior to the deltoid muscle. Note the consistent architecture of the biceps tendon; any disruption is indicative of an abnormality.
∗Images in this chapter courtesy of the University of Virginia Imaging Center, Charlottesville, Virginia.

Subscapularis
1. The patient should begin with the arm in a neutral position. As illustrated on the following page, return the transducer to the transverse orientation and image the axial biceps tendon, then move the transducer slightly superior and medial (toward the humeral head) to image the long axis of the subscapularis tendon. The image demonstrates how the long axis of the subscapularis tendon appears as a fibrillar band of medium level echoes posterior to the deltoid muscle. Dynamic imaging during internal and external rotation will provide full evaluation of the tendon. (S, Subscapularis tendon; BT, biceps tendon; D, deltoid muscle; C, coracoid process.)

2. With the patient still in the neutral position, rotate the transducer 90 degrees into the longitudinal plane, as illustrated below. The image demonstrates how the subscapularis tendon (S) will be seen in short axis just anterior to the humeral head (H). (D, Deltoid muscle.)

Supraspinatus
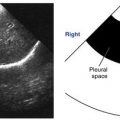
1. The patient should be placed into the Bouffard position with hand in back pocket and elbow extended posteriorly. In a slightly oblique transverse scanning orientation move the transducer laterally, superiorly and slightly posteriorly. The medial edge of the transducer will be pointing in the direction of the patient’s ear. The following image shows that in this plane the long axis of the supraspinatus tendon (SS) can be evaluated just anterior to the echogenic line of the humeral head (H). (D, Deltoid muscle.)

2. Maintaining the Bouffard position, the supraspinatus tendon should be evaluated in a longitudinal plane by rotating the transducer 90 degrees from the previous oblique transverse position. The critical zone of the rotator cuff is located here, about 1 cm lateral and posterior to the biceps tendon. (D, Deltoid muscle; H, humeral head; SS, supraspinatus tendon.)

Infraspinatus
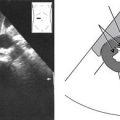
1. Return patient to neutral position. Turn the transducer to an oblique transverse orientation to align with the infraspinatus tendon. Move the transducer posteriorly and laterally just inferior to the spine of the scapula. The following image shows the deltoid muscle (solid arrow) anterior to the echogenic appearing infraspinatus tendon (dashed arrow). The echogenic line of the humeral head (dotted arrow) and scapula are posterior. Internal and external rotation or movement from neutral to hand reaching to opposite shoulder can be used for identification and evaluation.

2. Turn the transducer to an oblique longitudinal orientation. The following image shows the infraspinatus tendon (IT) between the medially placed glenoid (G) and the laterally placed humeral head (HH). (D, Deltoid muscle.)

Teres Minor
1. The patient should be in the neutral position. Return transducer to transverse position and move slightly inferior to image the trapezoidal shaped tendon in the long axis. The humeral head (HH) will be lateral and the deltoid muscle (solid arrow) anterior to the teres minor tendon (dashed arrow).

2. Turn the transducer to the longitudinal position to evaluate the tendon in the transverse axis.
Carpal Tunnel Scanning Protocol Overview
Location
Carpal tunnel region is located along the midwrist proximal to the crease toward the forearm and distal to the wrist crease toward the fingers.
Anatomy
• The carpal tunnel houses bones, tendons, nerves, ligaments, muscles and vessels, all providing the hand with the ability to function properly.
• The carpal tunnel consists of a bundle of tendons coursing from the flexor muscles in the forearm through the wrist and into the hand. At the level of the midwrist the superficial border to the tunnel is the transverse carpal tunnel ligament or flexor retinaculum. The tendons coursing through the tunnel are divided into 2 groups:
1. The more posteriorly situated tendons originate from the flexor digitorum profundus muscle in the forearm and travel through the tunnel to the fingers as the flexor profundus tendons.
2. The anteriorly placed tendons originate from the flexor digitorum superficialis muscle in the forearm and travel through the tunnel also to the fingers as the flexor superficialis tendons. The muscle and tendon aiding the first digit, or the thumb, originate from the flexor pollicis longus muscle on the radial side of the forearm. The tendons are all covered by a synovial sheath.
• The median nerve runs just anteriorly to the bundle of tendons and slightly toward the radial edge. The transverse carpal tunnel ligament or flexor retinaculum covers the tunnel transversely just anterior to the median nerve. The nerve is naturally elliptical in shape and will flatten slightly as it courses distally into the hand.
• The proximal carpal tunnel is located just before the crease in the wrist on the side of the forearm. Here, with the hand supinated, at the proximal region the pisiform stands as the bony landmark on the medial edge, scaphoid on the lateral edge, and lunate posteriorly. The profundus and superficialis tendons and median nerve are midline as described above. The flexor pollicis tendon courses laterally along the border of the scaphoid. Also at this level, the ulnar nerve and artery course along the medial edge adjacent and slightly anterior to the pisiform border. This anatomical area is known as Guyon’s canal. The carpal tunnel anatomy is draped anteriorly by the flexor retinaculum.
• The distal tunnel is located just past the crease in the wrist and is distinguished by the bony landmarks of the hamate medially, trapezium laterally and posteriorly by the capitate. The profundus and superficialis tendons continue along the middle of the tunnel with the flexor pollicis tendon far laterally along the border of the trapezium. The median nerve continues its course anteriorly and slightly laterally. All of these structures continue to be draped anteriorly by the flexor retinaculum.
Physiology
• The carpal tunnel houses the tendons that connect the muscles in the forearm to each of the digits in the hand. These tendons aid in movement of the fingers. Nerves coursing through the carpal tunnel, including the most prominent median nerve, provide sensation and muscle function to the fingers. These structures are surrounded by a tunnel of bones that provide stability, not only for the structures inside the carpal tunnel but to the entire wrist and hand.
Sonographic Appearance
• The tendons running midline through the carpal tunnel will appear hypoechoic compared to adjacent structures and will move with flexion of the fingers.
• The radial and ulnar arteries on the lateral and medial edges respectively, will appear anechoic and can prove to be a valuable landmark when color is used for identification.
• The median nerve coursing anterior to the tendons will also be hypoechoic relative to adjacent structures but the shape may be slightly elliptical and a thin hyperechoic ring can be seen around the periphery.
• Proximally, the echogenic curve of the bony surface of the pisiform on medial edge and scaphoid on the lateral edge is visualized. Moving distally, the bony surface of the hamate and trapezium, medially and laterally, respectively, can be located.
Preparation
Patient Prep
• No patient prep.
Transducer
• Linear 10 to 18 MHz.
Patient Position
• The patient should be sitting with the arm at 90 degrees and palm facing up in a resting position on a stable surface.
• A towel rolled and placed under the wrist can add stability and aid with neutral positioning of the anatomy.
Breathing Technique
• No breathing technique required.
Carpal Tunnel Survey
Transverse Plane
1. Toward the forearm side of the wrist place the transducer adjacent to the wrist crease to visualize the proximal carpal tunnel.
2. Identify the flexor superficialis and flexor profundus tendons midline and the flexor pollicis along the radial edge by having the patient flex the fingers. Identify the more hypoechoic median nerve (MN) anterior to the group of tendons.


3. This gray-scale version of color Doppler shows how it can be used to identify Guyon’s canal with the ulnar artery and nerve along the medial edge. (Dashed arrow: MN, Median nerve.)

4. Locate the midline posterior bony edge of the lunate. (Dashed arrow: MN, Median nerve.)

5. Move the transducer distally toward the fingers, staying adjacent to the crease of the wrist and angling slightly toward the proximal region.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


