Chapter 54
Nasopharyngeal Carcinoma with Pterygopalatine Fossa and Orbital Extension
Epidemiology
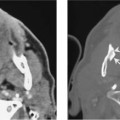
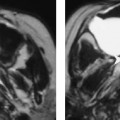
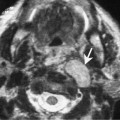
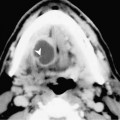
Nasopharyngeal carcinoma (NPC) often spreads anteriorly into the nasal fossa. This tumor may infiltrate the sphenopalatine foramen and extend through the pterygopalatine fossa in 15% of patients. In advanced cases, tumor may continue to spread into the orbital apex and subsequently through the superior orbital fissure into the intracranial cavity. NPC with intracranial extension may be seen in 31% of patients, but the most common route of spread is through the foramen ovale followed by direct tumor erosion through the skull base.
Clinical Findings
Involvement of the pterygopalatine fossa causes hypoesthesia or pain over the cheeks and this can be readily verified clinically by examining the cutaneous sensation over the distribution of the infraorbital nerve. The patient may also have concomitant weakness of the ocular muscles and diplopia.
Pathology
Tumor within the pterygopalatine fossa often usually widens the fossa, invades the pterygopalatine ganglion, or infiltrates the infraorbital nerve. Tumor may also spread intracranially via perineural involvement of the maxillary nerve and the nerve of the Vidian canal. Tumor in the orbital apex can cause dysfunction of the extraocular muscles. This is because Zinn’s ring (attachment of the extraocular muscles) is located in the orbital apex.
Treatment