Fig. 6.1
Diagram of the lateral skull for the common sites of cranial sonography through anterior (A), posterior (P), and mastoid (M) fontanelles
6.3.1.2 Normal Anatomy
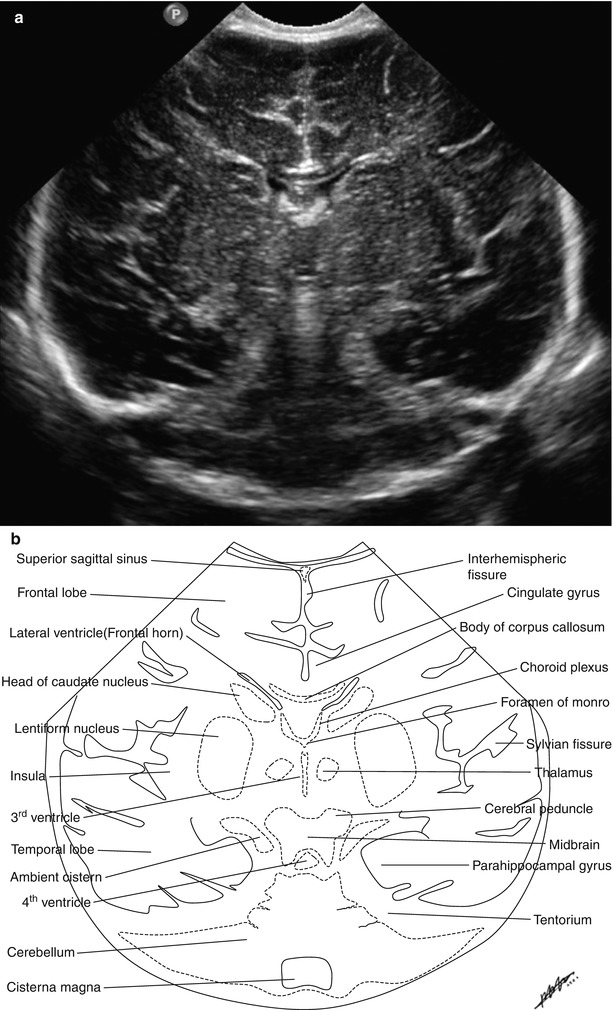
Fig. 6.2
(a and b) Coronal sonographic image (a) and schematic illustration (b) at the level of foramen of Monro through the anterior fontanelle
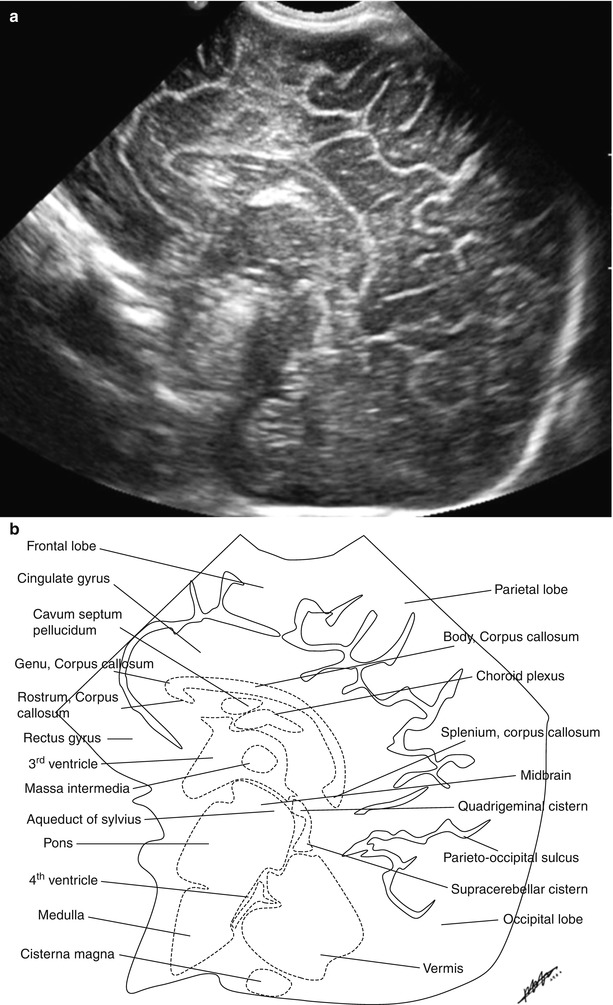
Fig. 6.3
(a and b) Midsagittal sonographic image (a) and schematic illustration (b) through the anterior fontanelle representing the whole corpus callosum, the third and fourth ventricles, brain stem, cerebellar vermis, and cistern magna
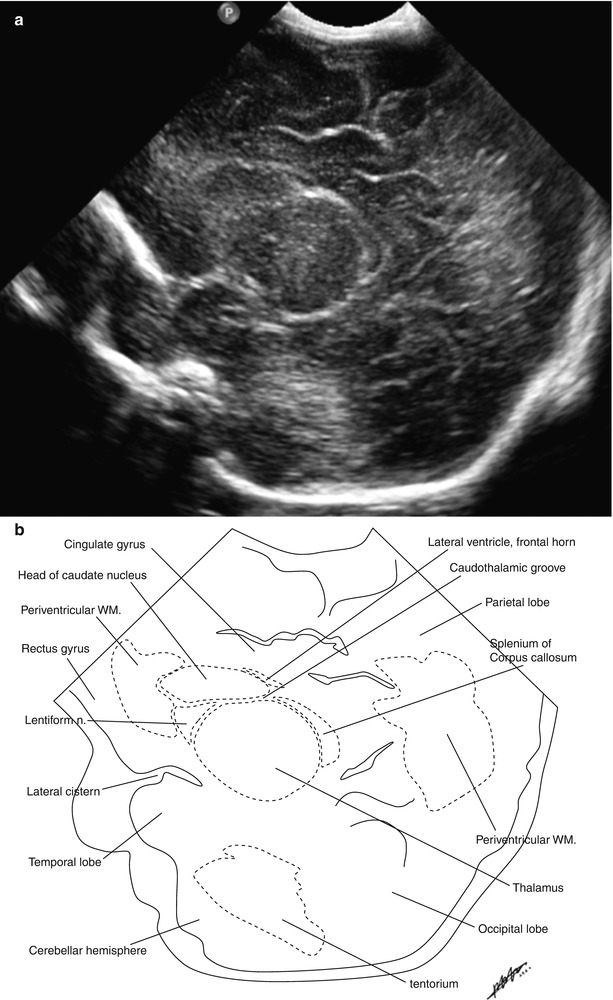
Fig. 6.4
(a and b) Right parasagittal sonographic image (a) and schematic illustration (b) at the level of the caudothalamic groove through the anterior fontanelle
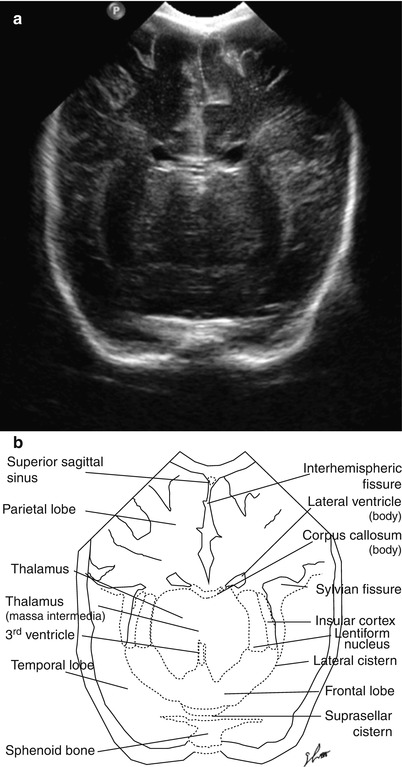
Fig. 6.5
(a and b) Coronal sonographic image (a) and schematic illustration (b) at the level of the bodies of the lateral and third ventricles through the posterior fontanelle
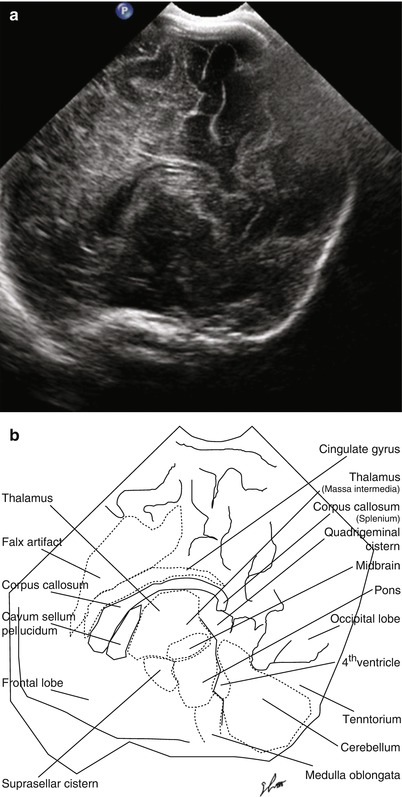
Fig. 6.6
(a and b) Midsagittal sonographic image (a) and schematic illustration (b) at the level of the corpus callosum and the third and fourth lateral ventricles through the posterior fontanelle
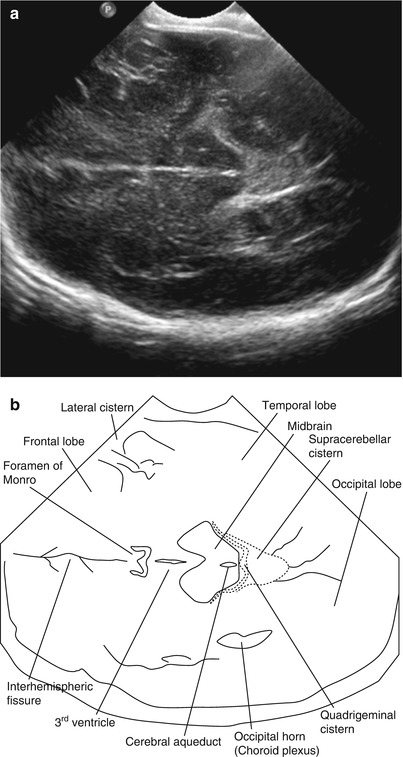
Fig. 6.7
(a and b) Oblique axial sonographic image (a) and schematic illustration (b) at the level of the third ventricle and midbrain through the mastoid fontanelle
6.3.1.3 Normal Variants and Pitfalls
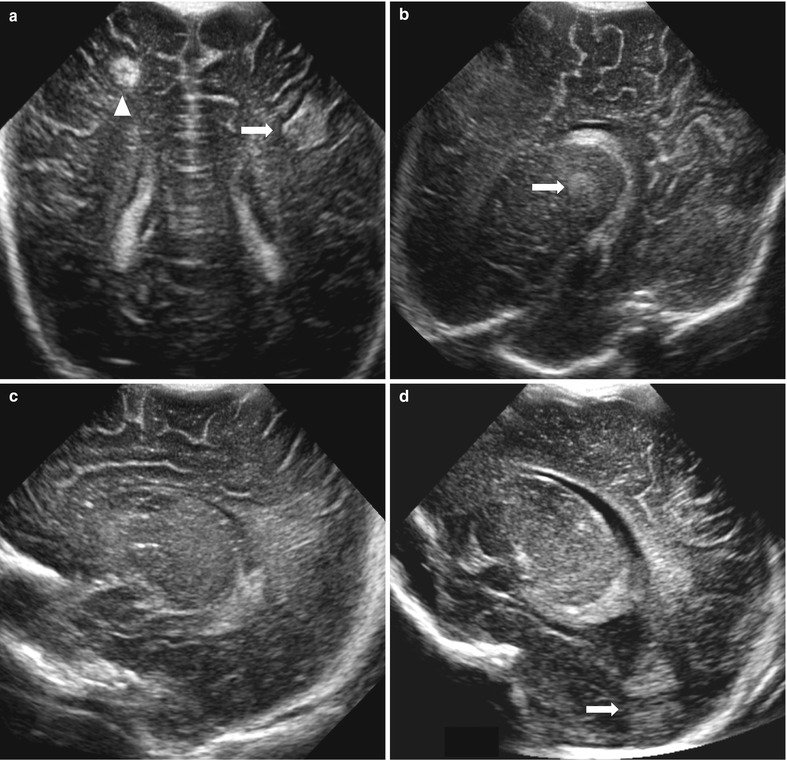
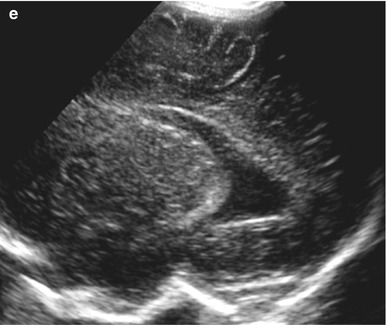
Fig. 6.8
Echogenic pseudolesion. (a) Posterior coronal scan through the anterior fontanelle in 1-day-old male neonate shows a triangular echogenic pseudolesion (arrow) in the left frontotemporal junction attached to adjacent sulci and a discrete, round echogenic lesion (arrowhead) in right frontal white matter apart from sulci confirmed as focal hemorrhagic infarct. (b) Left parasagittal scan through the posterior fontanelle in a 5-day-old male neonate shows a round echogenic density in the left thalamus (arrow), so-called thalamic pseudolesion. (c) On left parasagittal scan through the anterior fontanelle, thalamic pseudolesion disappeared. (d and e) Left parasagittal scan through the anterior fontanelle in a 2-day-old male neonate (d) shows a focal echogenic pseudolesion (arrow) posterior to dilated occipital horn of left lateral ventricle, and on left parasagittal scan through the posterior fontanelle (e), it disappeared
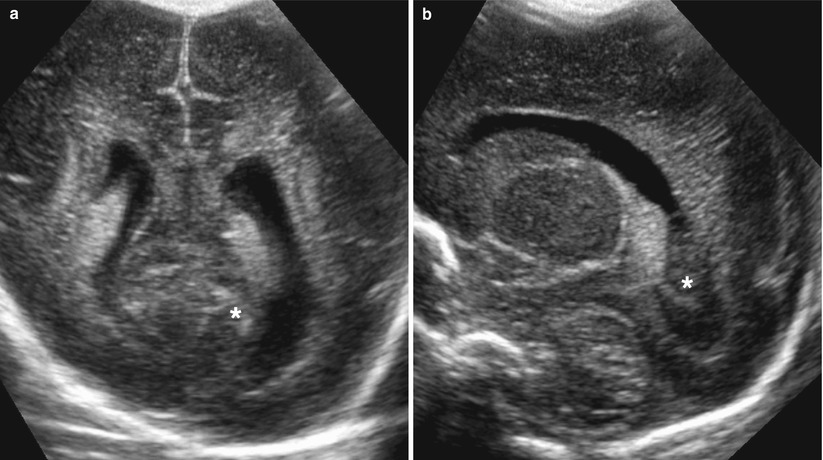
Fig. 6.9
Calcar avis in a 3-day-old female neonate. (a) Coronal image shows white matter mound by compression of medial side of lateral ventricle. (b) Left parasagittal image shows intraventricular hyperechoic mass in the occipital horn of the lateral ventricle mimicking intraventricular hematoma
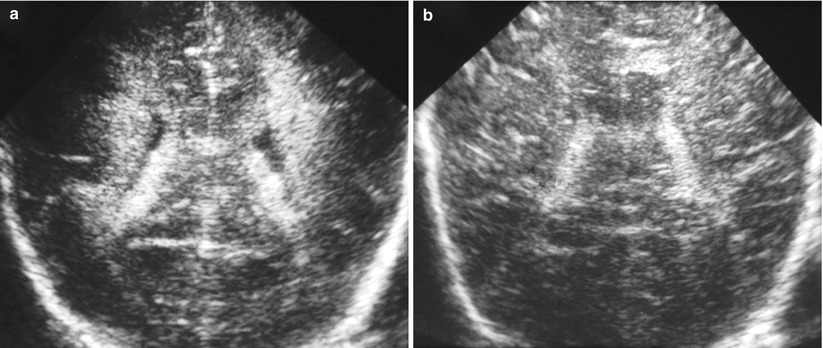
Fig. 6.10
Sequential changes of periventricular echogenic halo. (a) Coronal image of premature male infant at 30 weeks gestational age shows symmetrical, homogeneous, and high echogenic halos in both periventricular white matters. (b) Coronal image at 41 weeks of the corrected age shows near disappearance of both periventricular echogenic halos
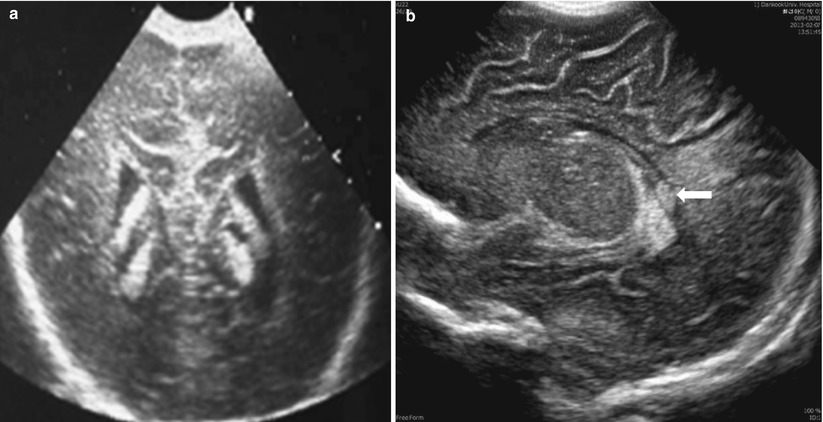
Fig. 6.11
Various patterns of normal choroid plexus. (a) Posterior coronal scan shows double patterns of choroid plexus in both lateral ventricles. (b) Parasagittal scan shows a nodular density (arrow) of the glomus
6.3.1.4 Germinal Matrix Hemorrhage
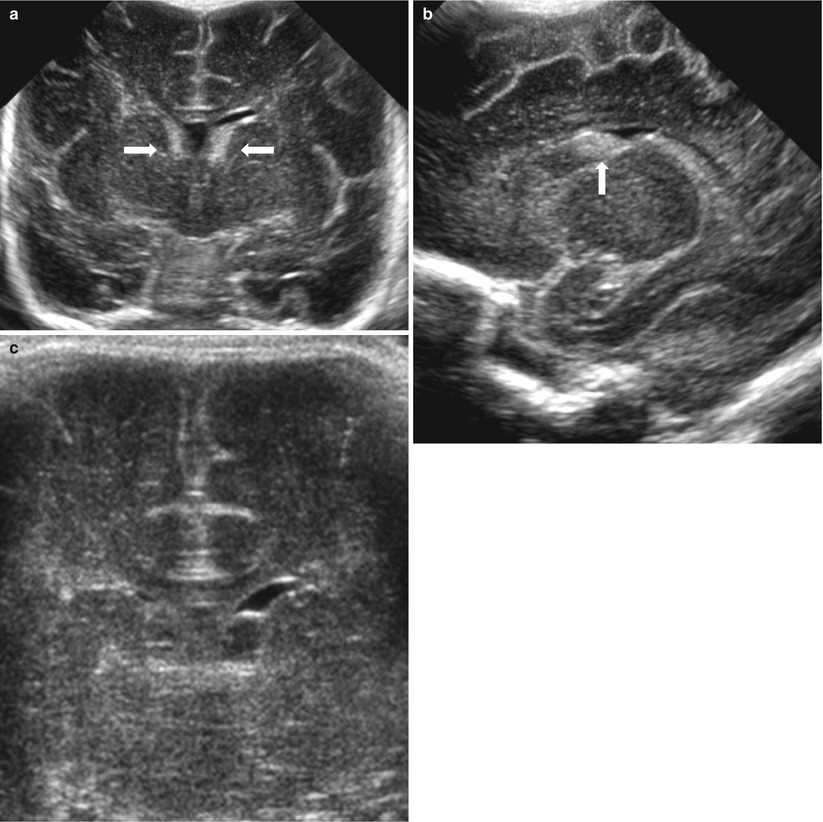
Fig. 6.12
Germinal matrix hemorrhage (GMH), Grade 1 in a 3-day-old female premature infant with 28 weeks gestational age. (a and b) Coronal (a) and right parasagittal (b) scans show ovoid-shaped-echogenic lesions in both caudothalamic grooves (arrows). (c) Follow-up coronal scan, 3 weeks later, shows cystic changes in both caudothalamic grooves
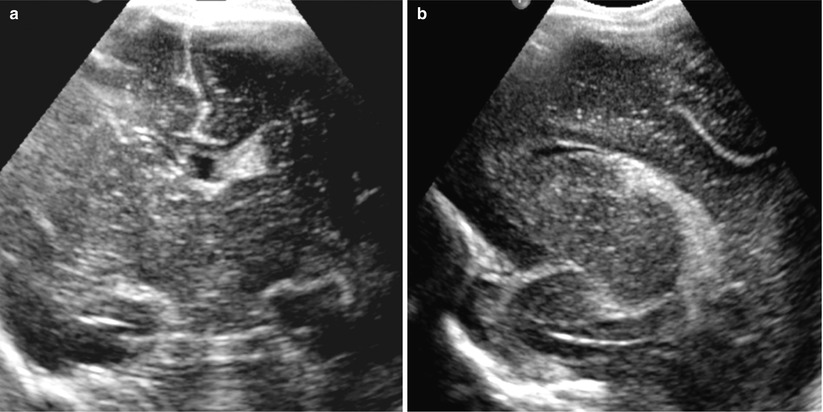
Fig. 6.13
GMH/IVH, Grade 2 in a 2-day-old female premature infant at 29 weeks gestational age. (a and b) Coronal (a) and left parasagittal (b) scans show echogenic materials in left caudothalamic groove extending into left lateral ventricle and no ventricular dilatation
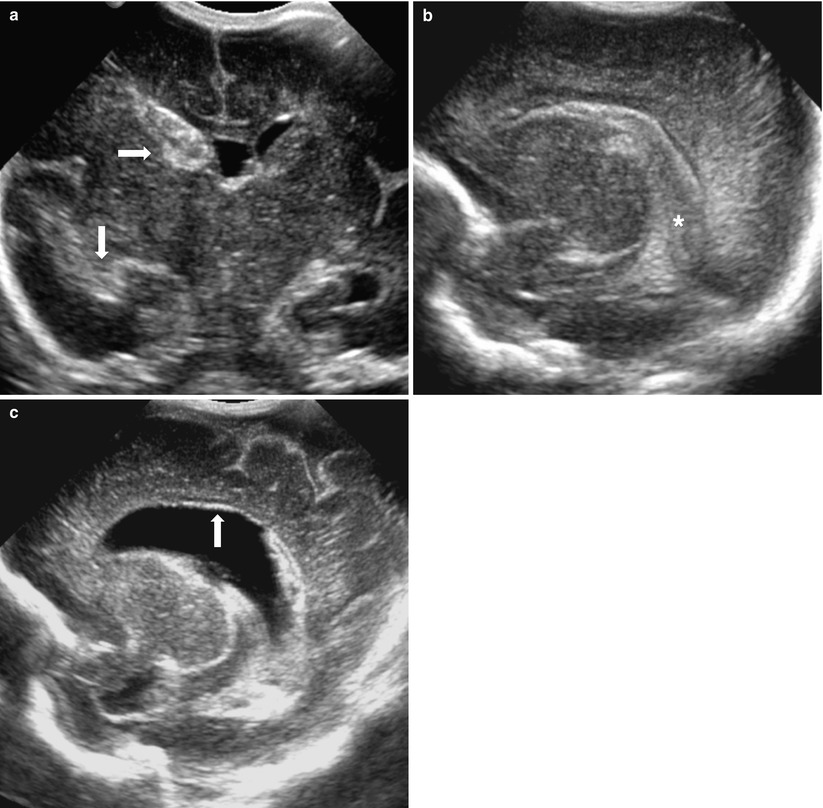
Fig. 6.14
GMH/IVH, Grade 3 in a 7-day-old female premature infant at 28 weeks gestational age. (a) Coronal scan shows large echogenic materials in right caudothalamic groove and temporal horn of right lateral ventricle (arrows) with dilatation of both lateral ventricles. (b) Right parasagittal scan shows echogenic materials in right caudothalamic groove extending into right lateral ventricle forming a cast of ventricular configuration. (c) Right parasagittal scan, 4 weeks later, shows progressive dilatation of right lateral ventricle, heterogeneous echogenic materials in right lateral ventricle suggesting residual blood clots, and increased ependymal lining echoes (arrow) along ventricular walls due to secondary ventriculitis
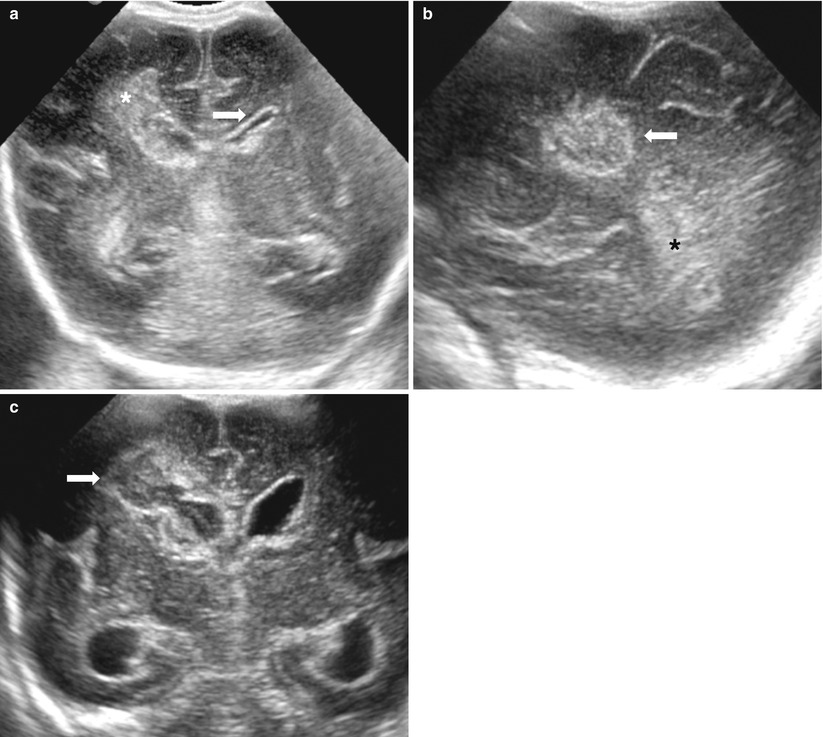
Fig. 6.15
GMH/IVH, Grade 4 in 1-day-old premature infant at 29 weeks gestational age. (a) Coronal scan shows echogenic materials in right caudothalamic groove extending into right frontal white matter and in left caudothalamic groove and both temporal horns of lateral ventricles with increased ependymal lining echoes (arrow). (b) Right parasagittal scan shows echogenic lesions in right frontal white matter as parenchymal hemorrhage (arrow) and in right lateral ventricle. (c) Coronal scan, 2 weeks later, shows cystic changes of right germinal matrix and parenchymal hemorrhage (arrow) and hydrocephalus
6.3.1.5 Intracranial Hemorrhage Except for GMH
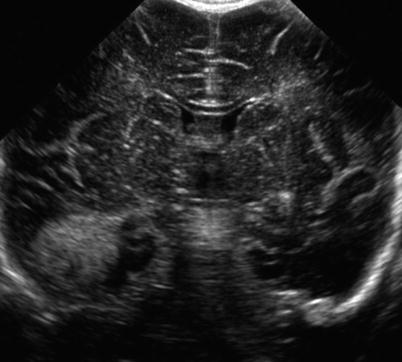
Fig. 6.16
Intracerebral hemorrhage in a 4-day-old female infant at 39 weeks gestational age. Coronal scan shows a round, discrete echogenic mass in right temporal lobe
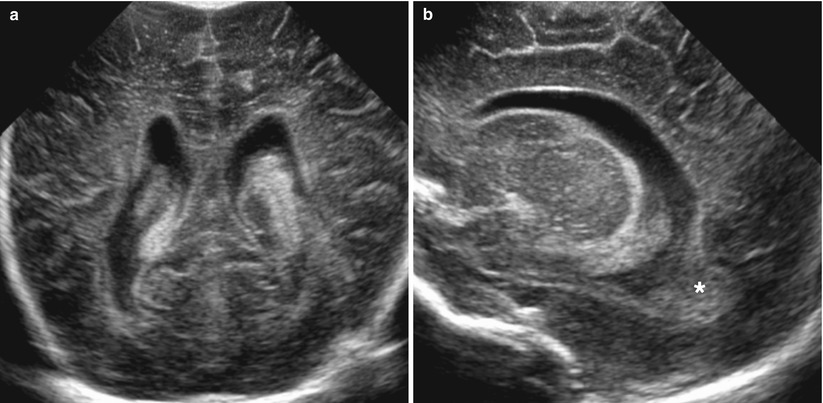
Fig. 6.17
Intraventricular hemorrhage in a 6-day-old infant with 36 weeks gestational age. (a) Posterior coronal scan shows heterogeneous echogenic lesions in both lateral ventricles with ventriculomegaly and increased ependymal echoes that cannot differentiate from normal choroid plexus. (b) Right parasagittal scan shows echogenic materials in posterior part of right lateral ventricle extending into the occipital horn representing as intraventricular hematoma
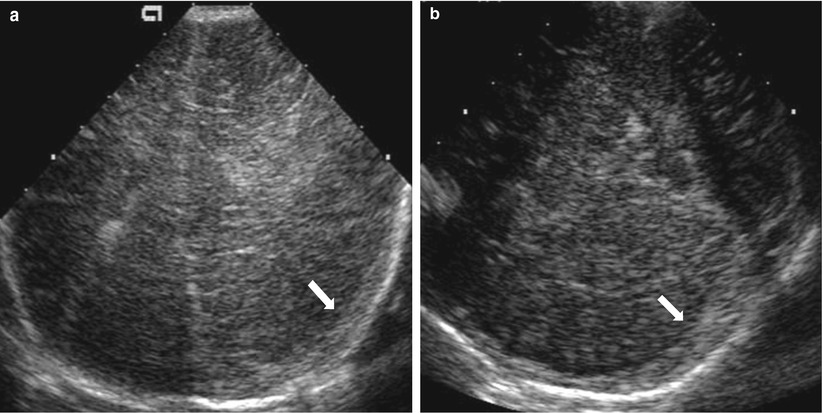
Fig. 6.18
Subdural hemorrhage and cerebral infarction in a neonate with hemophilia. (a) Coronal scan shows a crescent echogenic lesion along left cranial convexity (arrow) with increased echogenicities of the underlying parenchyma and ipsilateral mass effect. (b) Axial scan through right mastoid fontanels also shows a crescent, echogenic lesion along left cranial convexity (arrow)
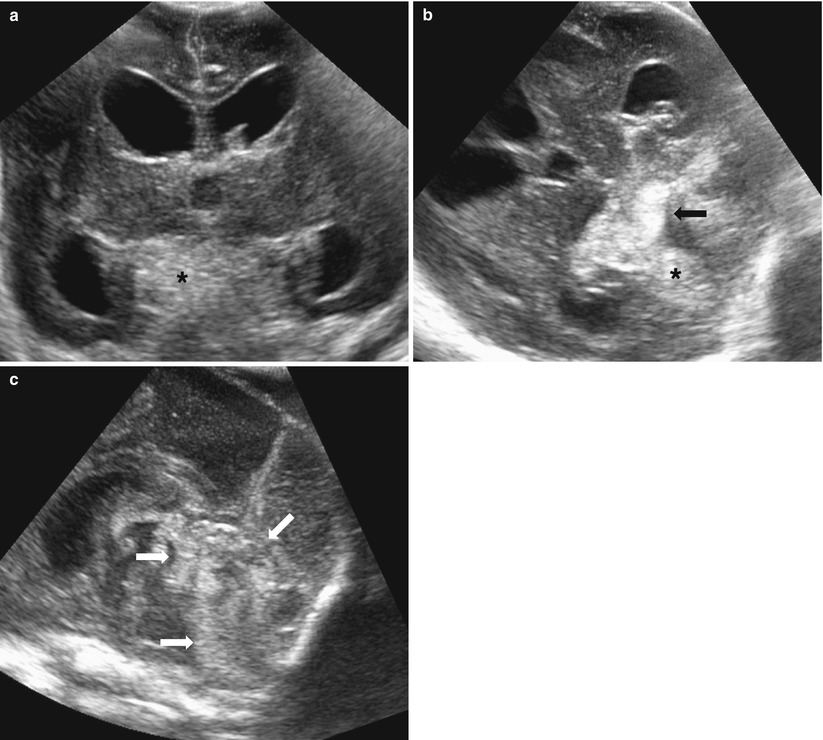
Fig. 6.19
Intraventricular and secondary subarachnoid hemorrhages in a 10-day-old premature male infant. (a) Coronal scan through the anterior fontanelle show various echogenic materials in the lateral, third and fourth ventricles, and posterior fossa with intraventricular obstructive hydrocephalus. (b) Axial scan through the left temporal fontanelle demonstrates large extent of echogenic materials in the lateral and fourth ventricles (arrow) as IVH and in posterior fossa as secondary subarachnoid hemorrhage flowing out from IVH. (c) Midsagittal scan through the posterior fontanelle shows heterogeneous echogenic lesions in the third and fourth ventricles, cisterna magna, and superior cerebellar cisterns (arrows) as the combined pattern of intraventricular and secondary subarachnoid hemorrhages
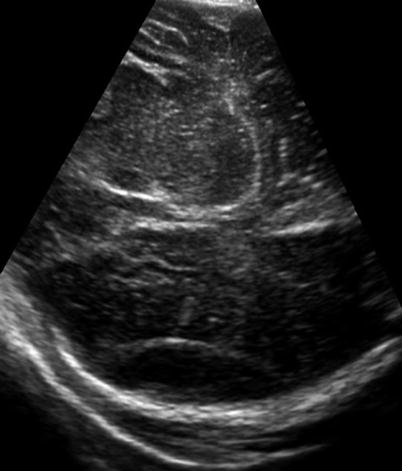
Fig. 6.20
Epidural hemorrhage in 1-day-old male term neonate with vacuum-induced vaginal delivery. Axial scan through the left mastoid fontanelle shows a lentiform, hypoechoic lesion along right parietal convexity with some echogenic debris and ipsilateral mass effect
6.3.1.6 Hypoxic-Ischemic Encephalopathy
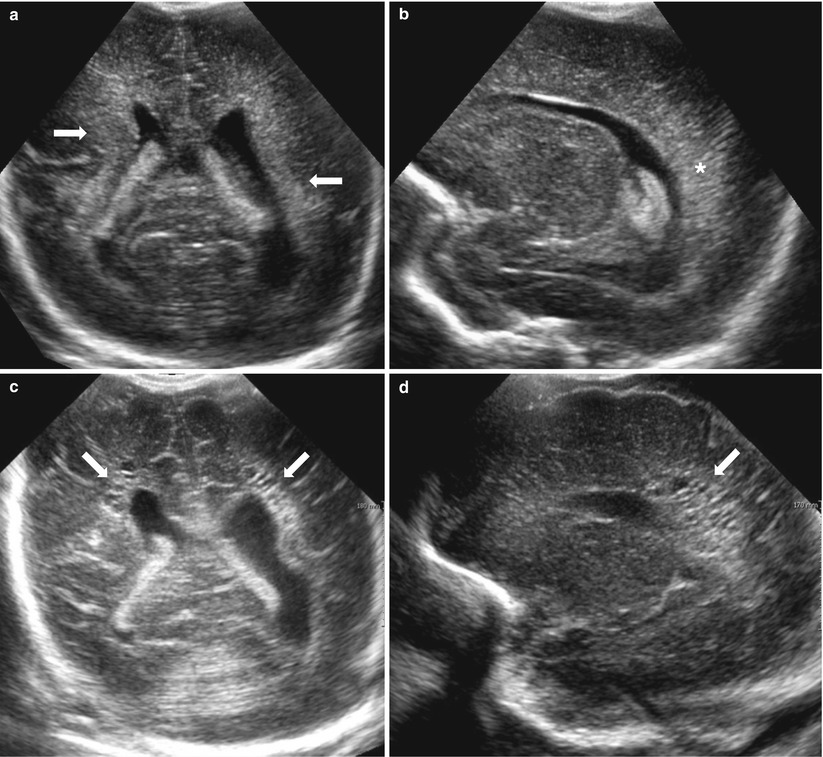
Fig. 6.21




Periventricular leukomalacia in a 3-day-old male premature neonate with 28 weeks gestational age. (a) Coronal scan shows discrete, extensive, and homogeneous echogenicities (arrows) in both periventricular white matters as well as the echogenicities of the corresponding choroid plexus. (b) Right parasagittal scan shows also discrete echogenicities in right peritrigonal white matter. (c and d) Follow-up coronal (c) and parasagittal (d) scans on 38 days later show multiseptate cystic lesions (arrows) in both periventricular white matters, especially peritrigonal areas that are confirmatory findings of periventricular leukomalacia
Related posts:


Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
