(1)
Department of Pediatric Radiology, University of Texas Medical Branch, Galveston, TX, USA
Abstract
The many normal variations which occur in the growing spine are dealt with in detail. These normal findings frequently are misinterpreted for abnormality, and just how to differentiate them from true abnormality is the main theme of this chapter.
Vertebral Bodies and Neural Arches
In the newborn and young infant the vertebral bodies, although basically rectangular, often appear more oval because they have rounded corners, especially anteriorly (Fig. 2.1a). Thereafter the vertebral bodies become more cuboid-rectangular (Fig. 2.1b), but in some individuals can appear exceptionally flat (Fig. 2.1c). The latter configuration is not to be misinterpreted as being representative of platyspondyly, as seen with bony dysplasias, for it merely reflects the wide spectrum of the normal appearance of the vertebral bodies.
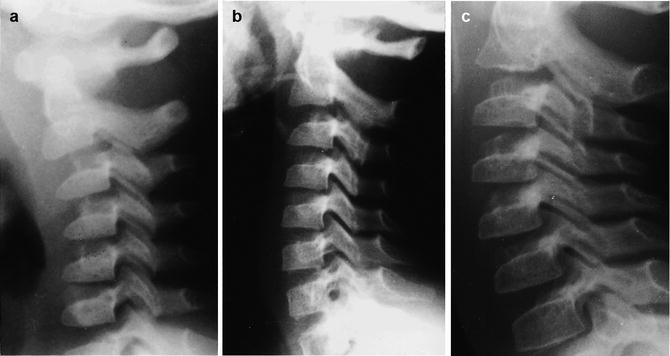
Fig. 2.1
Variable appearance of normal vertebral bodies. (a) In infancy the vertebral bodies appear more oval. (b) Typical appearance of rectangular-cuboid vertebral bodies in older children and adolescents. Note that there is some residual rounding of the upper anterior corner of C3. (c) In some patients, still normal, the vertebral bodies appear exceptionally flat
In the normal individual the neural arch of C2 usually is the largest such structure in the upper cervical spine. This is helpful when one is assessing radiographs for the presence of occipitalization. With occipitalization, C1 is fused to the base of the skull and yields to C2 as being the uppermost visualized posterior arch. Ordinarily it would be the second arch to be visualized. The posterior arch of C1 is smaller than the posterior arch of C2 and thus, when this arrangement is altered, and the uppermost visualized neural arch is the largest one present, one should suspect occipitalization.
In addition to the preceding considerations, the neural arches and spinous processes of the cervical vertebrae can show even more variation in configuration. In this regard, some may be hypoplastic, and in addition, while normal spinous processes tend to point downward, occasionally they point upward. Because of this they may erroneously suggest that a pathologic increase in the intraspinous distance is present (Fig. 2.2).

Fig. 2.2
Anomalous spinous tip configurations. Note the upward, pointing spinous tip of C4 (upper cross symbol). The spinous tip of C5 (X) points downward, as is more usual. However, one could misinterpret the combined findings as being representative of a flexion injury of the cervical spine, causing an increased intraspinous distance between C4 and C5
Finally, because of the complicated embryonic development of the cervico-occipital junction, aberrant bony ossicles frequently are encountered in the upper cervical spine and at the base of the skull. Most of these occur anteriorly, but they also can be seen posteriorly, and at either site usually are round or oval. Such ossicles have smooth edges and should not be misinterpreted for avulsion fractures (Fig. 2.3).
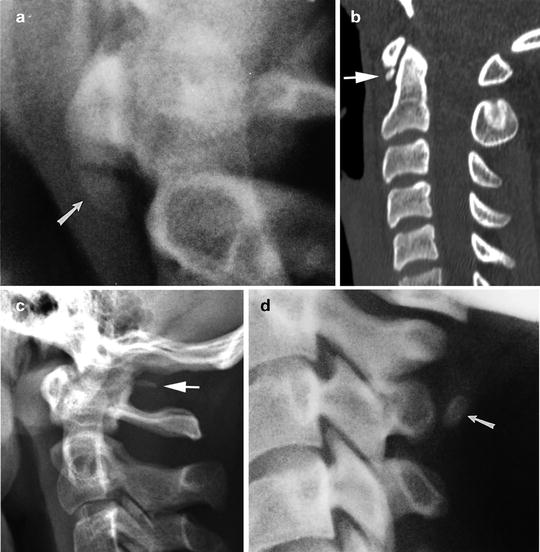
Fig. 2.3
Extra ossicles. (a) Note the extra ossicle (arrow) located below the anterior arch of C1. (b) In this patient, a small extra ossicle is seen along the inferior aspect of the anterior arch of C1 (arrow). (c) This patient demonstrates an extra ossicle in the posterior upper cervical region (arrow). (d) Note the extra posterior ossicle (arrow) at the C3 level. Also note that the neural arch of C3 is slightly deformed and hypoplastic (i.e., smaller than the other neural arches)
Normal Cervical Spine Motion Causing Pseudoabnormalities
In most individuals, flexion or extension of the cervical spine results in little excess motion. However, in other instances, and especially in infants and young children, since the ligaments are lax, normal physiologic hypermobility is more common and leads to spinal configurations that frequently are confused with pathologic states [1]. In addition, it is important to appreciate that the apex of the flexed cervical spine curve in infants and young children is located at a different level from that in older children and adults [2]. In infants and young children it is located in the upper cervical spine at approximately the level of C2–C3 (Fig. 2.4a), while in older children and adults it is located in the midcervical spine, that is, somewhere between C4 and C6 (Fig. 2.4b). This explains why cervical spine injuries, primarily flexion induced, are more common in the upper cervical spine in infants and young children, and more common at the C4–C6 level in older children, adolescents, and adults. This also is probably why degenerative changes in adults occur primarily at the C4–C6 level. In addition, when considered with the overall increased mobility of the infant’s and young child’s spine, it is more readily understood why so many normal hypermobility phenomena occur in the upper cervical spine in this age group.
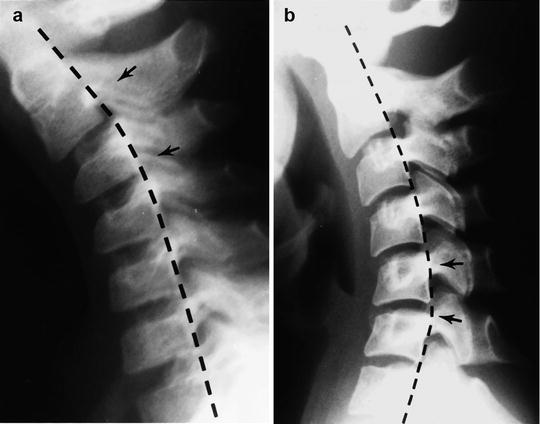
Fig. 2.4
Normal apex of flexion curve. (a) In infancy and young childhood, the apex of the flexion curve is at the C2–C3 level (arrows) (From Swischuk et al. [2].). (b) In older children and adolescents, the flexion curve migrates downward to a level somewhere between C4 and C6 (arrows)
High Anterior Arch of C1
This finding is common in young infants during hyperextension of the cervical spine [1]. The resultant configuration is that of a very high, indeed dislocated appearing, anterior arch of C1 (Fig. 2.5). The finding, to the uninitiated can be quite alarming but, is entirely normal.

Fig. 2.5
High anterior arch of C1. With hyperextension, the normal anterior arch of C1 (arrow) can assume a very high location. Indeed, it may appear that the cervico-occipital junction has been disrupted
Exaggerated C1–C2 Interspinous Distance
Similar to hypermobility of the anterior arch of C1, hypermobility of C1 with flexion can result in an exaggerated intraspinous distance between C1 and C2 [1]. However, as opposed to the high anterior arch of C1 phenomenon, this configuration also can be seen in older children. Indeed, distances of up to 10 or even 12 mm can be encountered and still be normal (Fig. 2.6). In these cases, however, the C1–dens distance (predental distance) is normal.

Fig. 2.6
Increased C1–C2 interspinous distance. Note the exaggerated, but normal distance (arrowhead to arrowhead) between the spinous tips of C1 and C2. Note that the predental distance is normal
C1-to-Dens (Predental Distance)
It is well known that the predental distance in infants and young children can be wider than in adults. Indeed, up to 5 % of normal individuals can demonstrate a predental distance of 5 mm, but most often the distance is somewhere between 2 and 3 mm on initial, neutral cervical spine studies [3, 4]. In any of these cases, if there is no increase in the predental distance on flexion, the finding can be considered normal (Fig. 2.7). However, it also should be recalled that with flexion there can be a normal increase in the distance of up to 2 mm (Fig. 2.8). If there is more widening than this, one should suspect underlying instability of the ligaments, either on a traumatic or congenital basis. The latter problem is associated with anomalies of the dens, primarily dens hypoplasia and an associated os odontoideum.
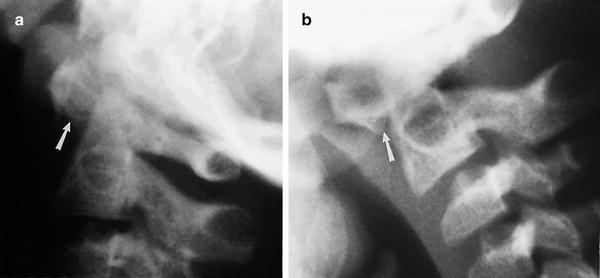
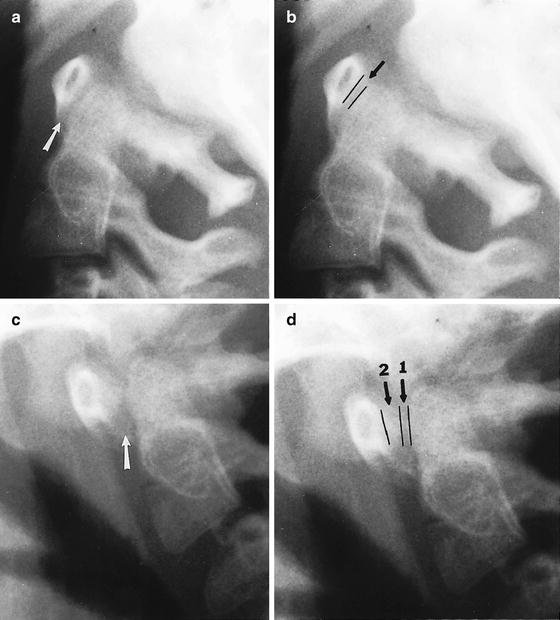
Fig. 2.7
Normal wide C1-to-dens distance. (a) Note the prominent C1-to-dens distance (arrow). The measurement was 5 mm. (b) On flexion, however, there is no increase in the distance (arrow). This patient was normal (Reproduced with permission from LE Swischuk, Emergency Imaging of the Acutely Ill or Injured Child, 4th ed. Lippincott Williams & Wilkins, Baltimore, 2000)
Fig. 2.8
C1-to-dens distance, maximum normal increase. (a) On extension, the C1-to-dens distance is normal. (b) The distance measures approximately 1–1.5 mm (lines). (c) On flexion, however, the predental distance increases (arrow). (d) Lines delineate the previous predental distance (1) and the new predental distance with flexion (2). Overall, the increase in distance with flexion is no more than 2 mm. Also note that the predental distance normally is slightly wider superiorly
Posterior Dislocation of Vertebral Bodies
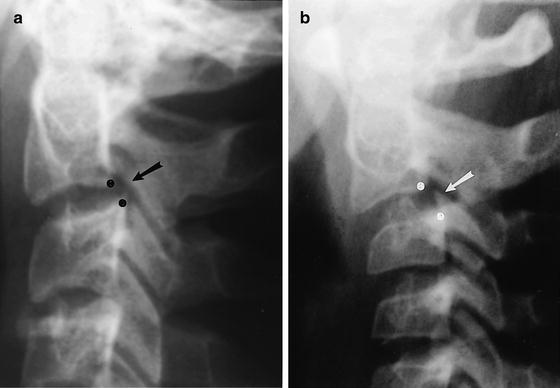
Physiologic posterior dislocation of the vertebral bodies occurs less frequently than anterior dislocation. It tends to occur over the midcervical spine, and maximum normal sliding should be no more than 2 mm [5]. The displacement can occur at one or multiple levels (Fig. 2.9).

Fig. 2.9
Normal posterior displacement of vertebral bodies (cross symbols). Note posterior displacement of C3 on C4 (upper arrow) and less, but still present, posterior displacement of C4 on C5 (lower arrow). This patient was normal
Anterior Angulation of C2 on C3
With spasm, or rigid positioning on an “EMS transporting backboard,” a patient’s head can be cocked forward so that angulation of C2 on C3 results [1]. In such cases there is no actual anterior displacement of C2 on C3, but the severe degree of angulation encountered can erroneously suggest that the ligaments between C2 and C3 have been disrupted and that dislocation is present (Fig. 2.10a). In these cases I have found it helpful to draw a line along the posterior aspect of C2 and the dens and note whether it intersects or just touches the upper posterior corner of C3. If it does, no dislocation is present (Fig. 2.10b). In such cases the posterior cervical line [6] should not be applied, for it will lead to erroneous conclusions. The line was designed to be used only if anterior displacement of the body of C2 on C3 was present (see next section).
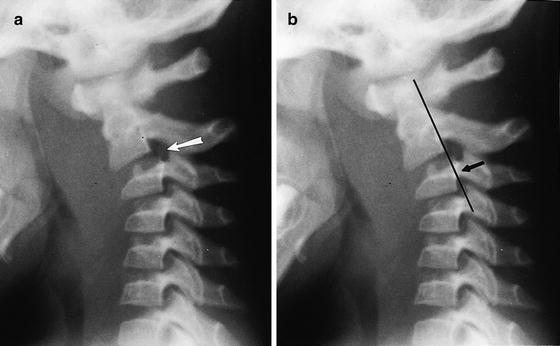
Fig. 2.10
Anterior angulation of C2 on C3. (a) Note that C2 is angled forward on C3 (arrow). (b) However, the line drawn along the posterior aspect of C2 does not intersect C3, but just touches the upper posterior corner of C3 (arrow). Therefore, there is no anterior dislocation. However, the prominent, but normal, C1-to-dens distance, generous C1–C2 interspinous distance, along with thickening of the soft tissues, due to improper technique, could lead one to erroneously diagnose a severe hyperflexion injury of the upper cervical spine
Anterior Dislocation of C2 on C3
Anterior dislocation of C2 on C3 can occur with a hangman’s fracture, but in infants and children it is far more common on a normal, physiologic basis [6, 7]. The degree of displacement is usually no more than 2 mm, but to the uninitiated a traumatic dislocation often is at first suggested (Fig. 2.11). In these cases I have found it helpful to apply a line, the posterior cervical line [6], to the anterior cortices of the spinous tips of C1 and C3, and then note whether it intersects, touches, or comes close to the anterior cortex of the spinous tip of C2 (Fig. 2.12). If the line misses the anterior cortex of C2 by more than 1.5 mm, a hangman’s fracture should be suspected. Otherwise, the finding should be considered physiologic (Fig. 2.13).
 < div class='tao-gold-member'>
< div class='tao-gold-member'>




Only gold members can continue reading. Log In or Register to continue
Related posts:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
