Case presentation
A 2-year-old child presents with difficulty ambulating for the past 24 hours. His parents state that the child has had fever, cough, and congestion for the past 5 days. He was seen twice by his primary care provider and diagnosed with a viral upper respiratory infection. A chest x-ray 1 day ago was interpreted as consistent with a viral process. The parents tell you that the child had had no bowel movement for the past 2 days, and today, in addition to his difficulty ambulating, he has not urinated. They also tell you that the child began to indicate soreness or discomfort in his arms and his legs.
Physical examination is remarkable for a quiet child, who, while not toxic, does not want to ambulate. He does not appear to be in obvious distress. He has a temperature of 102 degrees Fahrenheit and a heart rate of 130 beats per minute. His neurologic examination is significant for diminished strength throughout, although he is able to sit up. He appears to have equal tone. Reflexes are diminished bilaterally. Sensation is grossly intact. There are no rashes.
Imaging considerations
Computed tomography (CT)
CT of the brain may be helpful in patients who present with acute mental status changes or neurologic findings. This modality is useful at detecting intracranial masses and acute hemorrhage, is widely available, and does not require sedation in the majority of instances. However, the utility of CT is limited in the evaluation of neurologic symptoms where the etiology is suspected to be infectious, such as cerebritis or encephalitis, or inflammatory, such as demyelinating disorders. If a demyelinating disorder is suspected, CT is not the imaging study of choice.
Magnetic resonance imaging (MRI)
MRI is the modality of choice in patients whose neurologic symptoms are suspected to be due to an infectious etiology or a demyelinating disorder. MRI provides optimal imaging of brain and spinal cord anatomy, including gray and white matter as well as nerve roots. While the lack of ionizing radiation is advantageous, barriers to MRI use include the time necessary to complete a study and lack of immediate availability in many cases. In young children, sedation is often required to complete the study.
Imaging findings
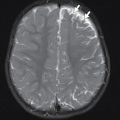
The child was admitted and MRI of the brain and spinal cord was obtained. Selected imaging is provided. Figs. 32.1 and 32.2 demonstrate abnormal T2 hyperintense signal of the central gray matter of essentially the entire spinal cord, most severe in the cervical spine.


Case conclusion
The child was admitted to the hospital with a diagnosis of acute flaccid myelitis (AFM). A lumbar puncture revealed mild pleocytosis and a negative Gram stain. On admission, consultation with Pediatric Neurology and Pediatric Infectious Disease was obtained and intravenous immunoglobulin (IVIG) and intravenous steroids were begun once the MRI and cerebrospinal fluid results were known. He was initially placed in a floor bed, but his weakness rapidly progressed and there was concern about his respiratory drive and he was transferred to the pediatric intensive care unit. Gradual improvement was noted. A repeat MRI on hospital day 9 showed significant improvement in previous abnormal cord signal with minimal residual T2 hyperintense signal, remaining most prominent in the upper cervical cord ( Figs. 32.3 and 32.4 ). At the time of discharge, the patient had improved motor strength but still had deficits. Follow-up with subspecialty services was arranged, including aggressive physical therapy with Pediatric Rehabilitation Medicine. He made a full recovery after 1 year of therapy.


Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


