Nuclear Medicine Procedures in the Pregnant and Lactating Patient
Nuclear Medicine Procedures in the Pregnant and Lactating Patient
Patrick M. Colletti
LEARNING OBJECTIVES
1. Describe the considerations for the use of radiopharmaceuticals in the pregnant patient.
2. Consult with the pregnant patients and their doctors regarding nuclear medicine procedures.
3. List nuclear medicine procedures never to perform during pregnancy.
4. Minimize the radiation exposure to the lactating patient and her child.
INTRODUCTION
It is of course reasonable to limit the use of radiopharmaceuticals in pregnant patients to situations where the potential benefits are greater than predicted fetal risks. Situations in pregnant patients arise in several scenarios. A patient may receive diagnostic or therapeutic radioisotope agents prior to the knowledge that she is pregnant, or she may receive a radioisotope scan to diagnose important conditions that occur during pregnancy. For example, the original use of placental scanning with 99mTc-human serum albumin was able to help locate the position of the placenta with the small estimated fetal dose <5 µGy (1). Nuclear medicine experts may be asked to estimate the risks for fetal injury associated with the radioisotopic procedure in question, including the possibility of consulting with the patient regarding potential recommendations for termination of the pregnancy.
WHAT ARE THE RISKS OF RADIATION IN PREGNANCY?
Potential risks for radiation to the fetus are difficult to differentiate from commonly occurring spontaneous fetal events. Table 19.1 summarizes the naturally occurring risks of common fetal adverse outcomes.
In addition to fetal loss, abnormal organogenesis, and intrauterine growth retardation, fetal radiation may be associated with postnatal malignancy. The background risk of childhood cancer mortality is 0.14%. The risk of childhood cancer death is thought to be 0.06% per 10 mGy in utero exposure (or 1/1700 additional cancers per 10 mGy). The lifetime risk of cancer is thought to be 0.4% per 10 mGy in utero exposure (3).
Table 19.1 SPONTANEOUS ADVERSE OUTCOMES OF PREGNANCY FROM WILCOX 1988 (2)
There are no convincing data linking medical imaging during pregnancy to adverse fetal outcomes. Brent (4) projected that diagnostic exposures to radiation presents a low risk, based on approximately 28.6% risk of spontaneous abortion, major malformation, mental retardation, and childhood malignancy among the general population that an exposure of 50 mSv (50 mGy) increases by approximately 0.17%.
Table 19.2 (5) presents recommendations for consulting with and advising pregnant patients regarding fetal risks associated with radiation exposure. In general, termination of pregnancy is not recommended unless there is reasonable documentation that an estimated fetal dose is greater than 150 mGy.
Radiopharmaceutical distribution and dosimetry in the pregnant patient
Fetal absorbed dose is the summation of external irradiation from maternal tissues as well as placental uptake and transplacental radiopharmaceutical transfer.
For radiopharmaceuticals excreted in urine, irradiation from maternal bladder may be the most important source. Hydration and frequent voiding may reduce the fetal absorbed dose significantly. Smaller administered dosages can significantly reduce the fetal absorbed dose at the expense of longer imaging times.
Lipophilic agents without significant albumin binding, with an molecular weight (MW) <500 to 1000 daltons (cut-off value 600 daltons) more likely cross the placental barrier. Large differences in amniotic structure and glucose transporter expression between animal models and the human placenta confound extrapolations of placental accumulation and transport. For reference, 18F-fluorodeoxyglucose (FDG) is 181 daltons (0.7 nm). As most available positron emission tomography (PET) radiopharmaceuticals are typically small molecules; 18F-FDG, Na18F, 82Rb, and 18F- Florbetapir would be expected to cross the placental barrier and directly irradiate the fetus.
Table 19.3 presents estimated fetal exposures associated with common routine dose nuclear medicine examinations (6,7,8). Table 19.4 correlates some of the limited newborn outcome data associated with nuclear medicine exams performed during pregnancy (9,10,11,12,13). Table 19.5 presents some of the case report information available regarding 18F-FDG PET/computed tomography (CT) in pregnant patients (14,15,16,17).
Table 19.5 FETAL ESTIMATED IRRADIATION FROM18F-FDG PET/CT CASE REPORTS (18)
6.7 mGy (reported combined maternal plus placental crossover)
3.9 mGy
10.6 mGy
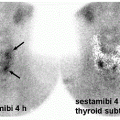
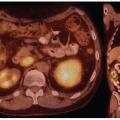
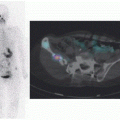
Radiopharmaceuticals that cross the placenta can be retained in the amniotic circulation. From here, the agent may be swallowed by the fetus and passed back into the amniotic fluid from where it may be re-swallowed and adsorbed or passed through again into the amniotic fluid. For example, Stabin et al. predicted that fetal exposure from 18F-FDG rises to 0.81 mGy/mCi up to 3 month and 0.61 mGy/mCi at 6 months to term when placental crossover is considered (18). Figure 19.1 demonstrates the mechanisms by which a fetus may receive radiation exposure. Figures 19.2 and 19.3 present an example of how PET/CT expose a fetus to radiation (17).
Imaging for suspected pulmonary embolism in pregnancy
Pregnant women are at two to four times the risk of pulmonary embolism (PE) compared with age-matched nonpregnant women. About 1 in 1000 pregnancies (19,20) may be complicated by PE, and PE is the cause of 20% of all maternal deaths (21). The clinical diagnosis of PE in a pregnant patient is particularly difficult because mild shortness of breath, elevated heart rate, and swollen legs are expected in late pregnancy, and Wells criteria and d-dimer levels may be unreliable in pregnancy (5). In view of the clinical problem of suspected PE in a pregnant patient, 2011 consensus guidelines from the American Thoracic Society and the Society of Thoracic Radiology along with the Society of Nuclear Medicine and Molecular Imaging and the American College of Obstetricians and Gynecologists recommend initial lower-extremity Doppler imaging and chest radiography followed by pulmonary CT angiography (CTA) if the chest radiographic findings are abnormal and ventilation-perfusion scintigraphy of the radiographic findings are normal (and in the absence of reactive airway disease). Follow-up is conducted with pulmonary CTA if the ventilation-perfusion findings are neither clearly positive nor clearly negative (22,23). Proceeding directly to pulmonary CTA is a credible alternative strategy (24,25,26,27,28).
FIG. 19.1 • Mechanisms of fetal radiation from PET/computed tomography (CT) or single photon emission computed tomography (SPECT)/computed tomography (CT). The total fetal radiation depends on radiation from isotope in placenta and surrounding tissues, radioactive urine in the maternal bladder, transplacental radiopharmaceutical transfer, and x-ray energy absorption associated with the CT. The relative exposures shown here may occur with typical fluorodeoxyglucose (FDG) positron emission tomography (PET)/computed tomography (CT).
Physiologic increased breast glandular tissue of pregnancy can cause increased breast radiosensitivity (28). CT strategies to reduce breast exposure should be considered (29).
Only gold members can continue reading. Log In or Register to continue