Occipital condyle/clivus/C1 vertebra metastasis – upfront stereotactic body radiation therapy
SKULL BASE REGION
Occipital condyle/clivus/C1 vertebra
HISTOPATHOLOGY
Papillary thyroid cancer
PRIOR SURGICAL RESECTION
No
PERTINENT LABORATORY FINDINGS
N/A
Case description
A 60-year-old female with a history of metastatic papillary thyroid carcinoma, who has been treated with lenvatinib for her systemic disease, presented with persistent headaches localized to the base of skull and upper neck, which was uncontrolled with medical management. Imaging with a positron emission tomography/computed tomography (PET/CT) scan and magnetic resonance imaging (MRI) revealed a focal area of increased activity within the right occipital condyle and a corresponding focal destructive lesion extending into the C1 vertebral body ( Figure 11.56.1 ).
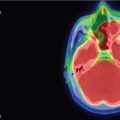
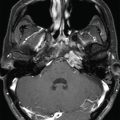
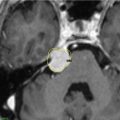
Figure 11.56.1.
A. Axial PET/CT scan image of the skull base demonstrating focal increased activity (SUVmax 10.4) in the right aspect of C1, corresponding to a focal destructive soft tissue lesion. B. Axial CT scan image of the skull base showing the focal destructive lesion with an extraosseous extension. C. Axial T1 postcontrast MRI of the skull base again showing the enhancing mass in the occipital condyle and C1 vertebral body.
Patient outcome
The patient completed stereotactic body radiation therapy (SBRT) to the base of skull without any acute treatment-related side effects ( Figure 11.56.2 ). She experienced symptomatic improvement at the treated site approximately 4 weeks following radiotherapy and was restarted on systemic therapy with lenvatinib. Follow-up imaging continued to demonstrate a partial response at the treated site ( Figure 11.56.3 ). She then developed symptomatic progression of her metastatic disease in multiple sites, including the clivus and multiple cervical vertebral bodies, for which she underwent a course of palliative external beam radiotherapy to a dose of 25 Gy in 10 fractions.
Radiosurgery Machine
CyberKnife
Radiosurgery Dose (Gy)
30 at the 77% isodose line
Number of Fractions
5
Figure 11.56.2.
Axial, sagittal, and coronal treatment planning CT images with corresponding isodose legend demonstrating the gross tumor volume (GTV) in shaded pink with a 1-mm expansion to the planning target volume (PTV). Surrounding critical organs-at-risk, including the brainstem (orange), are also outlined.
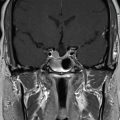
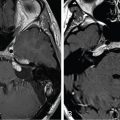
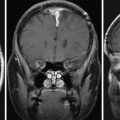
Figure 11.56.3.
A. Axial PET/CT scan image of the skull base performed approximately 6 months following SBRT, demonstrating a partial response to treatment with a substantial reduction in fluorodeoxyglucose (FDG) avidity at the treated metastasis. B. Axial postcontrast T1-weighted image of the skull base performed approximately 8 months following SBRT, demonstrating a partial response to treatment with significant reduction in the metastatic enhancement and reduction of the extraosseous disease. SBRT, Stereotactic body radiation therapy.
Critical Structure
Dose Tolerance
Brainstem + 1 mm PRV (planning organ-at-risk volume)
0.5 cc < 23.0 Gy
Max (0.03 cc) < 31.0 Gy
Cochlea
Mean < 10 Gy, ipsilateral
Mean < 5 Gy, contralateral
Spinal cord + 1 mm PRV
1.2 cc < 14.5 Gy
0.35 cc < 23.0 Gy
Max (0.03 cc) < 30 Gy
Globes
Max (0.03 cc) < 5 Gy
Optic nerves
Max (0.03 cc) < 5 Gy
Optic chiasm
Max (0.03 cc) < 5 Gy
Adjacent blood vessels
Max (0.03 cc) < 33 Gy
Only gold members can continue reading. Log In or Register to continue
Apr 6, 2024 | Posted by drzezo in GENERAL RADIOLOGY | Comments Off on Occipital condyle/clivus/C1 vertebra metastasis – upfront stereotactic body radiation therapy



 Esthesioneuroblastoma – delayed postoperative radiosurgery for recurrence at long-term
Esthesioneuroblastoma – delayed postoperative radiosurgery for recurrence at long-term
 Null cell – delayed postoperative radiosurgery for growing perioptic residual
Null cell – delayed postoperative radiosurgery for growing perioptic residual
 Chondrosarcoma – definitive radiosurgery after subtotal resections
Chondrosarcoma – definitive radiosurgery after subtotal resections
 Large vestibular schwannoma – delayed postoperative radiosurgery for growing residual
Large vestibular schwannoma – delayed postoperative radiosurgery for growing residual
 Trigeminal neuralgia due to petroclival meningioma – upfront radiosurgery
Trigeminal neuralgia due to petroclival meningioma – upfront radiosurgery
 Superior sagittal sinus meningioma – delayed postoperative, multisession radiosurgery for growing residual
Superior sagittal sinus meningioma – delayed postoperative, multisession radiosurgery for growing residual



