Opening Round

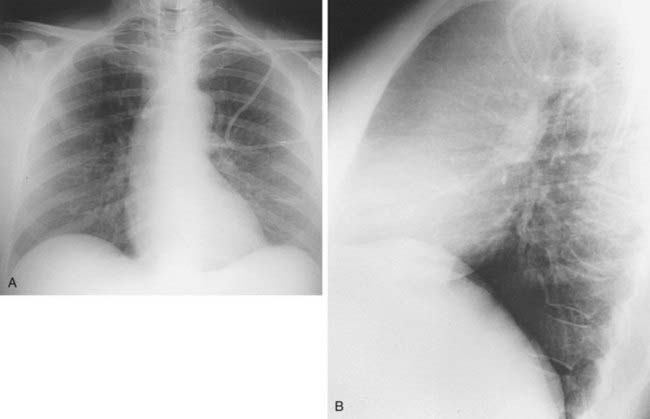
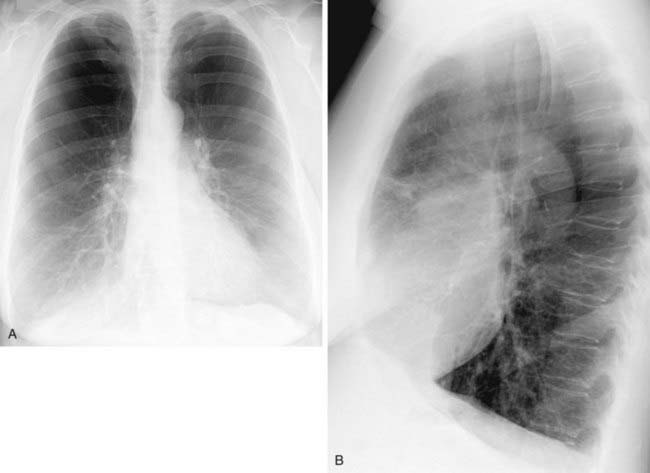
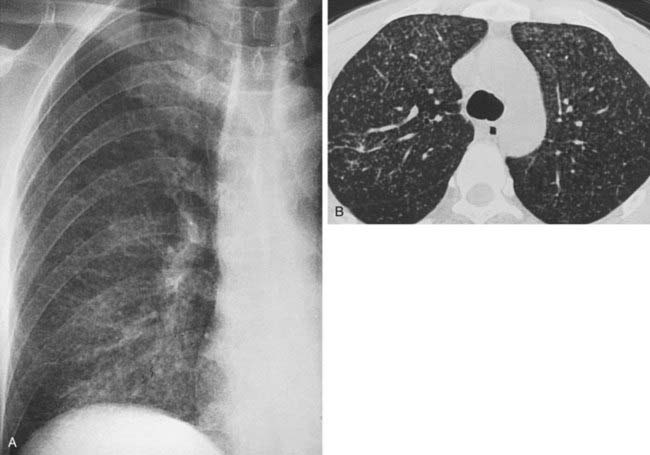
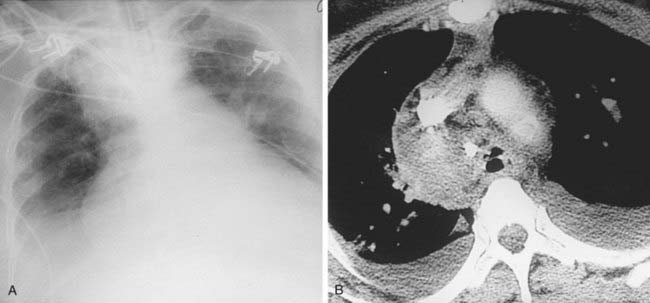
Spontaneous Pneumothorax Secondary to Ruptured Bleb
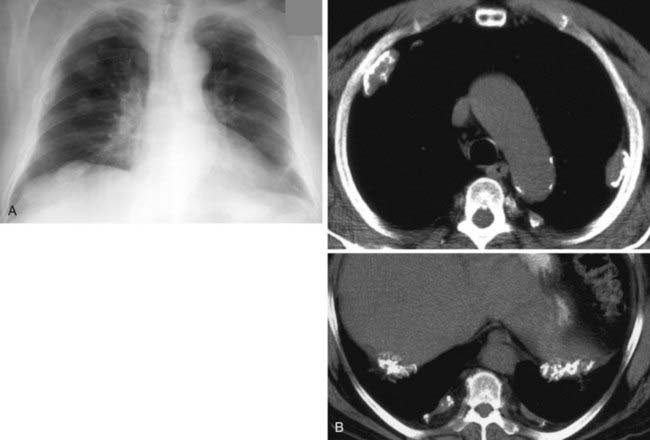
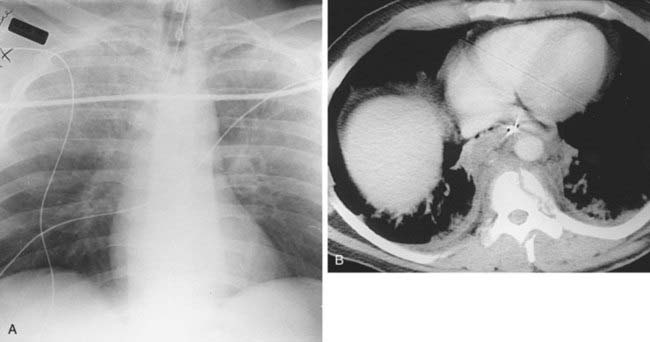
2 Spontaneous, chronic obstructive pulmonary disease, chronic infiltrative lung disease (e.g., Langerhans cell histiocytosis and lymphangioleiomyomatosis), malignant neoplasms (e.g., metastatic sarcoma), trauma, catamenial pneumothorax, iatrogenic, barotrauma, and infection (e.g., lung abscess and septic infarcts).