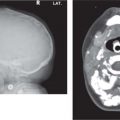
Radiograph/CT: Lytic destructive bone lesion with resorption of lamina dura resulting in floating teeth appearance. Associated heterogeneously enhancing soft-tissue mass.
Radiograph/CT: Radiolucent area traversed by t rabeculae forming various sized cavities. If trabeculae arranged in radiating pattern, then sunburst appearance.
Rare.
Rapid proliferation phase followed by slower involution phase.
Metastasis
Radiograph/CT: fairly well-defined, lytic mass with soft-tissue component.
Bone cyst due to trauma/injury
Radiograph/panorex: slightly irregular cyst with poorly defined borders and scalloped margins between the roots.
CT: Depends on fibrous vs osseous component. Varies from radiolucent to ground-glass.
Uni-/multilocular lesion, well-defined margin.
MRI: sharply demarcated mass, variable signal intensity, diffuse CE.
Pain, swelling, and displacement of teeth.
Active growth in childhood.
Malignant transformation in polyostotic variant described.
Fig. 4.150 Right mandibular bone destruction with floating tooth characteristic of Langerhans cell histiocytosis on 3D CT reconstruction of face.Fig. 4.151 Axial CT of mandible (bone window) showing a diffuse, expansile, ground-glass bone lesion with large osseous component on left, which is characteristic of fibrous dysplasia.
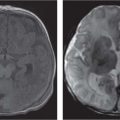
Radiograph: Poorly-defined destructive, mottled bone lesion with root resorption and loss of lamina dura of developing teeth. Associated cortical loss.
CT: destructive soft-tissue mass with extension into surrounding soft tissue.
MRI: diffuse infiltration, heterogenous mass with CE.
African variant most common childhood malignancy in Africa.
African Burkitt strongly associated with Epstein-Barr virus (EBV).
Radiograph/CT: Lytic destructive bone lesion with resorption of lamina dura resulting in floating tooth appearance. Associated heterogeneously enhancing soft-tissue mass. MRI: T1 iso-/hypointense mass, T2 hyperintense, variable CE.
Osteosarcoma
Radiograph/CT: lytic bone destruction with ill-defined margins (osteolytic type) or areas of sclerosis (o steoblastic type) with aggressive periosteal reaction, ± sunburst effect, ± cortical breakthrough, and ± calcification/osteoid formation.
MRI: heterogeneous mass.
NM: increased uptake, identifies other bone lesions.
Prone to recurrence and metastases.
Rhabdomyosarcoma
CT: Soft-tissue mass with variable but diffuse CE, ± bone erosion. May extend to involve mandible depending on site. MRI: T1 isointense, T2 hyperintense, variable but diffuse CE.
Forty percent occur in head and neck.
May extend intracranially.
Leukemia
Radiograph/CT: loss of lamina dura, varying degree of lytic bone destruction.
Radiograph/panorex: initially radiolucent then calcified, with the calcified portion separated from expanded cortex by a radiolucent zone ± impacted, unerrupted tooth.
Benign tumor made up of various components of teeth (enamel, dentin, cementum, pulp).
Located between roots of teeth.
May be associated with unerupted tooth.
Metastasis
Radiograph/CT: fairly well-defined, lytic mass with soft-tissue component.
Cementoma: cementifying fibroma
Radiograph/panorex: Early—well-circumscribed, well-demarcated radiolucent lesion with no internal radiopacities.
Well-defined, dense radiopaque material attached to tooth root with surrounding radiolucent zone.
Rare.
Mandibular first molar most frequently involved.
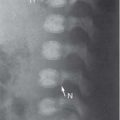
Fig. 4.152 Burkitt lymphoma with floating tooth and loss of lamina dura and cortical resorption on oblique radiograph of mandible.Fig. 4.153 Oblique radiograph of mandible showing expanded radio-lucent lesion with calcification and unerupted tooth consistent with an odontoma. Note how the calcified portion is separated from the cortex by a radiolucent zone.Fig. 4.154 Well-defined dense radiopaque material attached to tooth root is characteristic of a true cementoma on panorex view of the right mandible.
Radiograph: Poorly defined destructive, mottled bone lesion with root resorption and loss of lamina dura of developing teeth. Associated cortical loss.
CT: destructive soft-tissue mass with extension into surrounding soft tissue.
MRI: diffuse infiltration, heterogenous mass with CE.
African variant most common childhood malignancy in Africa.
CT: Depends on fibrous vs. osseous component. Varies from radiolucent to ground-glass.
Uni-/multilocular lesion, well-defined margin.
MRI: sharply demarcated mass, variable signal intensity, diffuse CE.
Camurati-Engelmann disease
Radiograph: sclerosis of base of the skull (BOS) ± cranial vault and facial bones.
Van Buchem disease
Radiograph: osteosclerosis and hyperostosis of mandible, endosteal sclerosis of cranium.
Fig. 4.155 AP radiograph of mandible shows diffuse periosteal thickening of mandible with dense laminated subperiosteal new bone formation, which is characteristic of Caffey disease.
Table 4.46 Congenital abnormalities: affecting size and symmetry
Diagnosis
Findings
Comments
Down syndrome
Radiograph: hypoplasia of the facial bones and sinuses, short hard palate, hypotelorism, dental abnormalities (delayed tooth eruption, anodontia).
Radiograph: premature closure any/all sutures, hypoplasia of the maxillomalar facial mass, recession malar bone, short and distorted zygomatic arches.
MPS (Hurler syndrome)
Radiograph: short wide mandible with obtuse angle, short rami, and flat/concave condyles. Premature closure of sutures, thickened calvarium at base, J-shaped sella.
Mandibulofacial dysostosis
Radiograph: hypoplasia/agenesis of malar bones, cleft palate.
Abnormality of first and second pharyngeal pouch, groove and arch structures.
Seckel syndrome
Radiograph: hypoplasia maxilla and mandible, microcrania, hypertelorism.
Fig. 4.156 Lateral radiograph of face shows mandibular hypoplasia in a patient with Pierre Robin syndrome.Fig. 4.157 Mandibular hypoplasia with absent angle of mandible in a patient with pyknodysostosis. Note the osteosclerotic bones on lateral radiograph of skull and face.
Only gold members can continue reading. Log In or Register to continue