Imaging Presentation
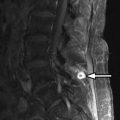
Computed tomography (CT) images reveal bone destruction of the C3 and C4 vertebral bodies and near complete collapse of the C4 vertebral body. There is a large area of tumoral bone formation along the left anterolateral aspect of the C4 vertebral body ( Fig. 57-1 ) . Magnetic resonance (MR) imaging revealed heterogeneous enhancement of a large paraspinal mass at C3-4 on the left with encasement of the left vertebral artery ( Figs. 57-2 to 57-4 ) . There was enhancing tumor extending into the left C3-4 neural foramen and into the epidural space anteriorly and on the left (see Fig. 57-4 ). The spinal cord was compressed from the left and displaced posteriorly and to the right by the epidural tumor (see Figs. 57-3 and 52-4 ). Surgery was performed to decompress the spinal cord and remove the tumor, which proved to be osteosarcoma. Because of the history of radiation therapy, this was presumed to be a radiation-induced vertebral osteosarcoma.




Discussion
Osteosarcoma, also known as osteogenic sarcoma , is a highly malignant primary tumor of bone that produces immature osteoid matrix. No more than 3% of osteosarcomas originate in the spine, so these are very uncommon vertebral tumors. Osteosarcomas represent up to 5% of primary malignant spine tumors, vertebral myeloma/plasmacytoma, and lymphoma being far more common. Most vertebral osteosarcomas manifest in the second through fifth decades of life. The much more common appendicular skeleton osteosarcomas usually occur in children or adolescents. Most primary vertebral osteosarcomas arise in the vertebral body but often infiltrate the pedicles and can involve the posterior arch. Only 10% to 17% of osteosarcomas are reported to occur primarily in the posterior vertebral arch. Primary vertebral osteosarcomas most commonly occur in the lumbar spine, followed by the thoracic spine, sacrum, and least commonly in the cervical spine. Most primary vertebral osteosarcomas have a bulky, lobulated soft tissue component that breaks through the cortex and commonly extends into the spinal canal or paraspinal soft tissues (see Figs. 57-1 to 57-4 ).
The majority of vertebral osteosarcomas are metastatic tumors that originate from primary osteosarcomas in the appendicular skeleton or adjacent soft tissues of the extremities in children, adolescents, or young adults ( Figs. 57-5 to 57-7 ) . These patients often have hepatic and pulmonary metastases in addition to vertebral metastases.


Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


