Fig. 17.1
Rotavirus encephalitis. (a–c) At day 3 after hospitalization, DWI demonstrates obvious high signals at the left cerebral hemisphere, the white matter of bilateral frontal lobes, and dental nucleus. (d–f) At day 10 after the onset, DWI demonstrates absence or shrinkage of the above lesions, with no newly formed lesions (Reproduced with permission from Kubota T, et al. Brain Dev, 2011, 3 (1): 21)
Case Study 2
A boy aged 4.5 years experienced vomiting and diarrhea for 2 days. Following examinations demonstrated rotavirus antibodies in the stool specimens. At days 3–4 after the onset, the boy experienced loss of consciousness for 10–20 s with accompanying sursumversion and following influent speech. At day 7 after the onset, the cerebrospinal fluid examination demonstrated protein 0.25 g/L, glucose 3.28 mmol/L, and rotavirus antibody negative, while MR imaging demonstrated no abnormality.
Fig. 17.2
Rotavirus encephalitis. (a) At day 29 after the onset, coronal T2WI demonstrates increased signals at the bilateral cerebellar cortex. (b) At day 93 after the onset, sagittal T1WI demonstrates broadened cerebellar sulci (Reproduced with permission from Shiihara T, et al. Brain Dev, 2007, 29 (10): 670)
Case Study 3
A boy aged 2 years was hospitalized due to sudden disturbance of consciousness after diarrhea and vomiting for 2 days. Rotavirus antibody was detected in the stool specimens. By laboratory tests, Na was 56.55 mmol/L and Cl was 91 mmol/L. EEG demonstrated intracerebral diffuse slow waves. Both cerebrospinal fluid examination and brain CT scanning demonstrated no abnormality.
For case detail and figures, please refer to Fukuada S, et al. Pediatr Neurol, (2009), 40 (2): 131.
17.7.2.2 Guillain-Barre Syndrome
MR neuroimaging demonstrates lesions at the nerve roots, ganglia, and nerve trunk area. Coronal imaging demonstrates typical cases with bilaterally symmetrical frog sign. The sign is possibly related to neural inflammatory edema and inflammatory cell infiltration, especially macrophage infiltration, demyelination, and angiopathies (including congestion at the intraneural vessels and perineural vertebral venous plexus, hyperplasia of small vessels, and inflammatory cell infiltration). The pathogenesis of the frog sign still needs to be clarified based on scientific studies.
Plain imaging demonstrates the cases of acute GBS with different degrees of thickening of involved spinal nerves and cauda equina. In some cases, the thickening is demonstrated as thickened both anterior and posterior roots, while in some other cases, thickening is demonstrated only as thickened anterior root. T1WI demonstrates moderate signals, while T2WI demonstrates moderate or slightly high signals. Contrast imaging usually demonstrates slight or obvious enhancement, with different degrees of enhancements for the same one patient. Coronal imaging demonstrates cord-like enhancement of the involved cauda equina. Transverse imaging demonstrates round, oval, or aggregated patches of enhancement. Sagittal imaging demonstrates backward aggregation of cauda equina, which is located at the middle and posterior lumbar spinal canal.
Based on the different ways of enhancements of the nerve roots, Ali Yikilmaz et al. classified these enhancements into four types: no enhancement, more obvious enhancement of the anterior root than the posterior root, same enhancement of the anterior root as the posterior root, and only enhancement of the anterior root.
17.7.3 Intussusception
17.7.3.1 Ultrasound
Transverse ultrasonography demonstrates high and low alternatively mixed echo area and its surrounding ring-shaped low-echo area. Otherwise, round-shaped center (liquid dark area) with homogeneous high echo is demonstrated, namely, the concentric ring sign or target ring sign. Vertical ultrasonography demonstrates similar signs to transverse ultrasonography, with the invaginated segment in round headlike structure and its surrounding low-echo area, namely, the sleeve sign. The thicker outer layer is demonstrated with lower echo, indicating more severe edema at the intestinal wall of the intussusception part. The ileum-type intussusception or ileocolon-type intussusception can be demonstrated as typical triple-ring sign with the intestinal cavity liquid as the background. The inner ring is the proximal intussusceptum segment; the middle ring is the distal intussusceptum segment; and the outer ring is the distal intestinal segment. Due to special features of pediatric small intestinal intussusceptions, small intestinal pneumatosis occurs. Therefore, high-frequency ultrasonography should be performed to improve the resolution power and achieve favorable demonstration of the small intestinal intussusception. And the diagnostic rate can thus be improved.
17.7.3.2 X-Ray
Abdominal X-ray for erect and supine positions is an essential routine examination before enema for children with intussusception. Its use facilitates the observation of pneumoperitoneum, intestinal obstruction, abdominal effusion, and preoperative gas distribution, which guide air enema diagnosis and reduction of the small intestine. Only about 10 % of the cases can be directly demonstrated with intracolonic soft tissue lump.
17.7.3.3 CT Scanning
CT scanning can demonstrate the characteristic sleeve sign and sausage sign as well as the particular stripe-shaped masslike thickening at the mesenteries. CT scanning plays an important role in defining the occurrence of intussusception, location and degree of intussusception, as well as the complications of intestinal ischemia, necrosis, and strangulation. In particular, CT scanning can accurately define the diagnosis of small intestinal intussusception.
17.7.3.4 Electronic Colonoscopy
By electronic colonoscopy, after the gas injection, semispherical or cervix-shaped intussusceptal head can be demonstrated in the colonic cavity, which moves along with the pressure of gas injection. It can also be performed to observe the mucosa in the enteric cavity as well as to assess intestinal ischemia and necrosis.
17.7.4 Other Related Syndromes
17.7.4.1 Reye Syndrome
CT Scanning
CT scanning demonstrates mostly diffuse cerebral edema as low-density lesions at the basal ganglia, brainstem, and cerebellum. The density of the periventricular white matter is demonstrated with obvious decrease, which extends bilaterally towards the frontal lobe and the temporal lobe in a butterfly shape. After that, the low-density areas bilaterally penetrate into the cortex from the frontal lobe and temporal lobe like a deer horn. The cerebral ventricle is subject to deformity due to compression.
MR Imaging
In addition to diffuse cerebral edema, T1WI, T2WI, and FLAIR all demonstrate no abnormality. Otherwise, T2WI demonstrates high signals at the basal ganglia, brainstem, and cerebellum. For some patients, special changes can be radiologically demonstrated. It has been reported that some of the low-density lesions at the brainstem and thalamus demonstrated by CT scanning were in high signals by T1WI and T2WI. It has also been reported that MR imaging demonstrated diffuse changes at the cortex and white matter, which were laminar high T2WI signal along cortex at the acute stage, with enhancement by contrast imaging; diffuse cortical high T1WI signals at the chronic stage. Meanwhile, changes of white matter and cerebral atrophy can be demonstrated.
Mao YL et al. reported MR imaging demonstrations at the acute stage. The cases with high T1WI, T2WI, and FLAIR signals of scattering spots of lesions at the cortex and subcortex, with enhancement of the lesions by contrast imaging, are suspected to be intracerebral adipose deposition. The cases with equal T1WI signals as well as high T2WI and FLAIR signals of scattering flakes of lesions at the cortex and subcortex are suspected as cellular edema. By contrast imaging, marginal enhancement of the lesions is demonstrated, which supports the diagnosis of destructed blood-cerebrospinal fluid barrier caused by mitochondrial dysfunction of local vascular endothelial cells. The above two types of demonstrations may be found overlapping.
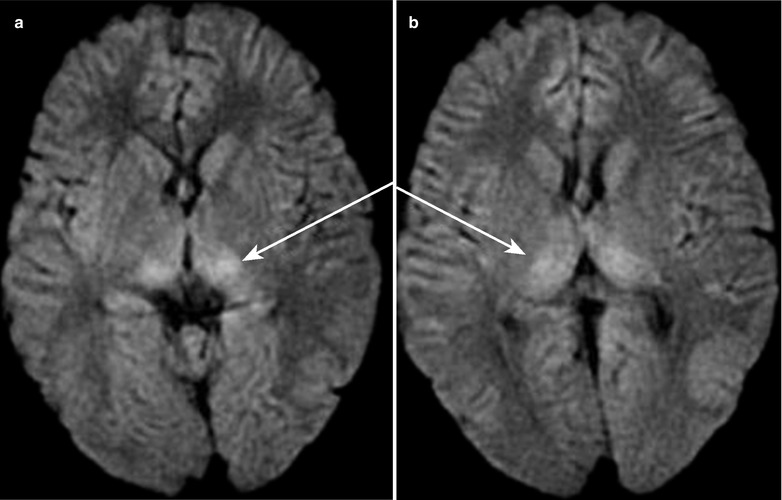
DWI is more sensitive to cerebral lesions than routine MR imaging, and, therefore, DWI can detect those cerebral lesions that routine MR imaging fails to demonstrate. DWI demonstrates most cases with high signal lesions at the whiter matter of thalamus, midbrain, and cerebellum (Fig. 17.3). DWI occasionally demonstrates high signal lesions at the whiter matter of subcortex and nearby sagittal sinus.
Case Study 4
A boy aged 5.5 years complained of altered mental status after vomiting and respiratory tract infection for 2 days. Laboratory tests demonstrated decreased blood glucose, AST 7125–9893 U/L, blood ammonia 204 μmol/L, and prolonged prothrombin time. Head CT scanning demonstrated mild cerebral edema.