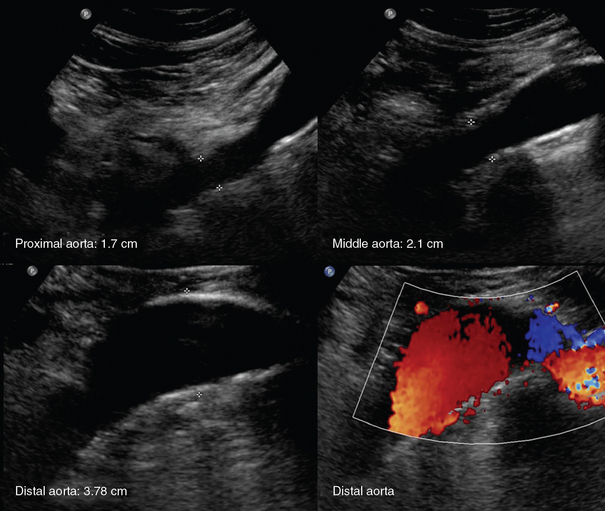
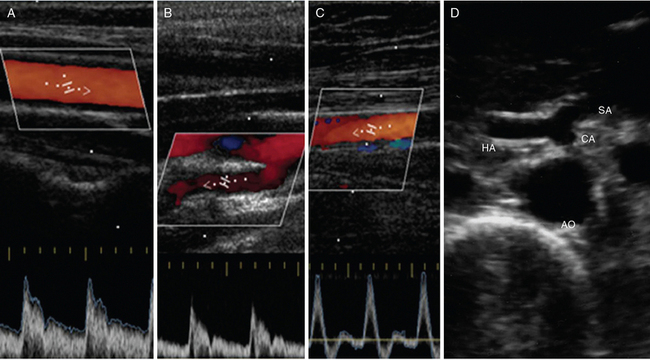
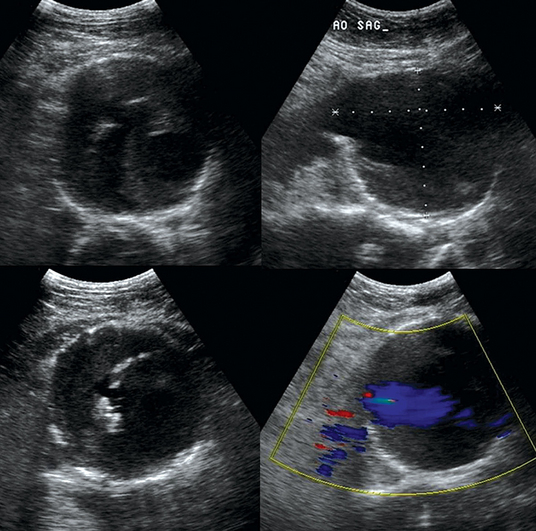
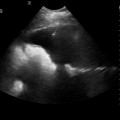
8 Procedural and diagnostic vascular ultrasound applications are essential in the intensive care unit (ICU). This chapter presents a synopsis of arterial disorders, whereas evaluation of venous thrombosis and ultrasound-guided vascular procedures are presented in Chapters 9 to 18. The left-sided aorta couples the left ventricle to the arterial system. Transthoracic ultrasound detects the ascending aorta (left parasternal view) and the aortic arch (suprasternal view). In the ICU, however, these acoustic windows may be impossible to obtain. Transesophageal echocardiography (TEE) is invaluable in visualizing the thoracic aorta in the ICU but typically cannot image the entirety of the thoracic aorta. Usually, the brachiocephalic trunk, left common carotid artery (CCA), and left subclavian artery (SCA) originate from the arch, in that order. The right CCA begins at the bifurcation of the brachiocephalic trunk, whereas the right vertebral artery (VA) originates from the right SCA. One third of patients have a common origin of the left CCA and brachiocephalic trunk, or the former originates from the proximal segment of the latter. The left VA may originate from the arch, and the right SCA may exhibit an aberrant origin. A right-sided aorta is rare and frequently associated with other types of congenital cardiovascular disease.1,2 The CCA is detected sonographically in the lateral aspect of the neck by using high-frequency transducers (7.5 to 10 MHz) in both the longitudinal and transverse planes. The CCAs run upward to about the upper border of the thyroid cartilage before branching. The normal Doppler spectral waveform (DSW) of the CCA has a narrow peak systolic and forward diastolic flow (Figure 8 E-1). The CCA bifurcates into the internal (ICA) and external (ECA) carotid arteries. The ICA does not branch in the neck and has a low-resistance DSW with forward diastolic flow. The ECA branches in the neck and has a high-resistance DSW with reversed diastolic flow. The VA runs toward the sixth cervical vertebra and enters the base of the skull accompanied by its vein. The SCA becomes the axillary artery after crossing the first rib, and the latter continues as the brachial artery (BA) after the posterior axillary fold. The BA ends about 1 cm distal to the elbow by dividing into the radial artery (RA) and ulnar artery (UA). The RA becomes the deep and the UA the superficial palmar arch, respectively, which join in the hand. The DSW of upper extremity arteries is triphasic. Figure 8 E-1 Normal Doppler spectral waveform of the common carotid artery (A), internal carotid artery (B), and superficial femoral artery (C). D, Abdominal aorta (AO) giving off the celiac artery (CA), which branches into the splenic artery (SA) and hepatic artery (HA). The descending thoracic aorta is detected sonographically via the cardiac apical window. The abdominal aorta (AA) begins at the aortic hiatus of the diaphragm and ends at the fourth lumbar vertebra (bifurcation). The AA is detected sonographically on longitudinal, transverse, and oblique planes by using convex transducers (2.5 to 5 MHz), and its DSW is biphasic. The AA gives off several main branches: the celiac artery (CA), which supplies the liver, gallbladder, stomach, intestines, and pancreas and in turn branches into the splenic, left gastric, and common hepatic arteries (see Figure 8 E-1); the superior mesenteric artery (SMA), which originates approximately 1 cm inferior to the CA and supplies the intestines and pancreas; the inferior mesenteric artery (IMA), which supplies the colon and rectum; and the renal arteries, which branch off last and supply the kidneys and adrenal glands. The AA bifurcates into the right and left common iliac arteries at the level of the umbilicus, and these vessels travel distally to divide into the internal (IIA) and external (EIA) iliac arteries. The EIA enters the thigh at the inguinal ligament and becomes the common femoral artery (CFA). The CFA bifurcates into the superficial (SFA) and deep (DFA) femoral arteries. The DFA travels laterally and medially to supply the deep thigh muscles. The SFA travels distally through the adductor canal (Hunter canal) into the popliteal fossa and becomes the popliteal artery (POPA). The POPA gives off several branches (e.g., sural) and bifurcates into the anterior tibial artery (ATA) and the tibioperoneal trunk (TPT). The ATA travels anteriorly and laterally between the tibia and fibula and becomes the dorsalis pedis artery (DPA) as it travels across the foot. The TPT bifurcates into the posterior tibial artery (PTA) and peroneal artery. The PTA travels posterior to the medial malleolus and peroneal artery and down the calf. The PTA bifurcates into the medial and lateral plantar arteries in the foot. The latter join with the plantar metatarsal arteries to form the plantar arch. The lower extremity arteries have a triphasic DSW (see Figure 8 E-1).1,2 An aortic aneurysm is defined as aortic dilatation (diameter >1.5 times the normal aortic diameter), and rupture of it is associated with high mortality. Aneurysms result from weakening of elastin and collagen within the medial layer of the arterial wall. A thoracic aortic aneurysm (TAA) resembles a mediastinal mass. Use of TEE and computed tomography (CT) is often necessary for accurate diagnosis. TAAs are commonly thrombosed and saccular. An abdominal aortic aneurysm (AAA) is the most common type of aortic aneurysm and is qualitatively defined as having a diameter greater than 3 cm (Figures 8 E-2 and 8 E-3). The AA has no vasa vasorum to facilitate repair; moreover, the ratio of elastic fibers to collagen changes from 3.1:1 in the proximal ascending aorta to 2.8:1 in the midthoracic region to 0.8:1 in the AA. AAAs are true aneurysms (fusiform, saccular) and can remain asymptomatic. They are usually atherosclerotic and infrarenal and have a predicted expansion rate of 0.2 to 0.5 cm/yr. Mild aortic dilatation (>2.0 and <3.0 cm) is described as ectatic, a moderate AAA is 3 to 5 cm in diameter, and a severe AAA is larger than 5 cm and corresponds to increased risk for rupture necessitating surgical repair (>80% mortality). In the ICU, surface ultrasound could be a useful examination to evaluate the aorta, although several limitations such as obesity, edema, abdominal gas, and trauma may hinder proper evaluation. Regardless, the vast majority can be imaged if alternative views such as coronal scanning through the liver are used when needed. Indications for performing ultrasound examination of the AA are surveillance of a known AAA, detection of an abdominal bruit on auscultation, unexplained shock, abdominal pain, pulsatile aorta or mass, history of hypertension or smoking, age older than 50 years with a family history of AAA, aneurysm in another vessel, aortic coarctation, lower extremity arterial disease, and the presence of emboli in the absence of another source. Ultrasound can be used to estimate the anteroposterior and transverse AAA diameter from outer wall to outer wall (Figure 8-1). The DSW through an AAA may reveal systolic dampening and diastolic reversal along with swirling of blood flow. A thrombus (mural or circumferential), usually of mixed echogenicity, or atherosclerotic plaque (hyperechoic areas confined to the aortic wall) may be found. Rupture or leakage is indicated by depiction of free fluid in the abdominal spaces, particularly retroperitoneal hematoma. Contrast-enhanced CT is used to confirm the findings and is the method of choice for diagnosis of leakage.1,3 Figure 8-1 Huge infrarenal abdominal aortic aneurysm (anteroposterior diameter, 7.5 cm) with a mural thrombus and calcifications (top: transverse and sagittal views; bottom: transverse views).
Overview of the arterial system
The arterial system
Disorders

Related posts:
 Ultrasound-guided peripheral intravenous access
Ultrasound-guided peripheral intravenous access
 Ultrasound-guided arterial catheterization
Ultrasound-guided arterial catheterization
 Ultrasound-guided placement of inferior vena cava filters: (CONSULTANT-LEVEL EXAMINATION)
Ultrasound-guided placement of inferior vena cava filters: (CONSULTANT-LEVEL EXAMINATION)
 Use of ultrasound in the evaluation and treatment of intraabdominal hypertension and abdominal compartment syndrome
Use of ultrasound in the evaluation and treatment of intraabdominal hypertension and abdominal compartment syndrome
 Ultrasound imaging in space flight
Ultrasound imaging in space flight
 Procedural ultrasound for surgeons: (CONSULTANT-LEVEL EXAMINATION)
Procedural ultrasound for surgeons: (CONSULTANT-LEVEL EXAMINATION)
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Overview of the arterial system