Pancreas: Differential Diagnosis of Pancreatic Diseases
10.1055/b-0034-87863
Pancreas: Differential Diagnosis of Pancreatic Diseases
Sonography is the modality of choice for the initial evaluation of suspected pancreatic disease in children because ionizing radiation is not involved and sedation is not required. Pancreatic magnetic resonance imaging (MRI) is indicated after suboptimal or equivocal US findings and a high clinical suspicion of pancreatic pathology. Although not recommended as the initial routine imaging study for the pancreas, CT is useful when sono-graphic findings are not diagnostic, the MRI is not available, and, also, for guidance of diagnostic and therapeutic procedures (aspiration biopsy, drainage, etc.).
Diffuse Pancreatic Involvement
Table 2.15 Normal-sized pancreas
Diagnosis
Findings
Comments
Preterm or term healthy newborn
The echogenicity of the pancreas in most cases is similar to that of the liver, although it can be less or more echogenic in premature and term newborns during the first 4 wk of life.
Cystic fibrosis
In first stages, when complete pancreatic replacement by fat without fibrosis is visualized.
On US, the pancreas is hyperechoic (echogenicity similar to that of the retroperitoneal fat) but unchanged in size.
Exocrine pancreatic insufficiency that leads to mal-absorption, with normal results on the sweat test, short stature, and bone marrow dysfunction. The characteristic pathologic finding is fatty infiltration of the pancreas
Johanson-Blizzard syndrome
The pancreas can show complete fatty replacement similar to Shwachman-Diamond syndrome.
CT: low-attenuation tissue interposed between normal pancreatic parenchyma.
On MRI, the fatty infiltrated pancreas has a signal intensity higher than the normal pancreas on in-phase T1-weighted images and loss of signal intensity on opposed-phase T1-weighted images.
The pancreatic body and tail are the dominant areas of fatty replacement.
Other storage diseases (hemosiderosis)
Similar to fatty infiltration. MRI: loss of signal intensity related to normal pancreas on gradient-echo T2-weighted sequences.
Structural change due to hemosiderin deposition.
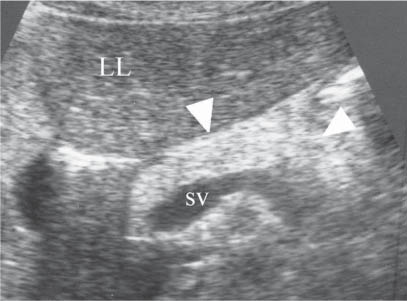
Fig. 2.25 Shwachman-Diamond syndrome. Transverse sonogram shows a pancreas of normal size with increased echogenicity similar to that of the retroperitoneal fat (arrowheads).
The most common US finding is diffuse/focal glandular enlargement and decreased echogenicity with poorly defined borders.
CT shows diffuse pancreatic enlargement, heterogeneous attenuation (there is a striking decrease or total lack of enhancement, related to the development of pancreatic zones of ischemia and necrosis), a poorly defined pancreatic contour, and peripancreatic fluid, that are most commonly found in the anterior pararenal space and lesser sac. More than a third of patients with acute pancreatitis have an initially normal CT.
Clinical entity caused by a wide variety of etiological agents: viral infections, drugs, and hereditary abnormalities. Trauma is the most common cause in children.
Infiltration in malignant diseases (Burkitt lymphoma, leukemia)
Diffuse pancreatic enlargement is the second pattern in frequency (15%–44% of cases). Pancreatic contour may be smooth or lobulated. The next most frequent US pattern is diffuse in almost all cases, other abdominal organ involvement is present: lymphadenopathies, bowel wall mass, and/or visceral tumoral infiltration (kidneys, liver, etc.).
Non-Hodgkin lymphoma is the most frequent tumoral pancreatic disease in children, involving the pancreas secondarily in approximately 30% of patients with widespread disease.
Metabolic diseases
Hyperlipidemia, hyperparathyroidism.
Fig. 2.26 Acute pancreatitis. Focal acute pancreatitis in a 3-year-old girl with acute abdominal trauma. Sonogram shows a pancreatic head (h, between calipers) of increased size and normal hypoechogenicity.Fig. 2.27 Burkitt lymphoma. A diffuse pancreatic involvement in Burkitt lymphoma. CT image shows homogeneously increased size of the pancreas (arrows).
The classic sonographic findings are an increase in the echogenicity and a decrease in pancreatic size with the typical fine-lobular (cobblestone-like) normal echo pattern of the pancreas no longer detectable. Complete pancreatic atrophy without any fatty replacement can also be found. In those cases, the pancreas shows a decreased size with normal echogenicity.
On MRI: soft-tissue attenuation without scattered areas of fat attenuation or high signal intensity.
Calcifications and multiple cysts within the pancreas can also be found.
The most significant autosomal recessive pancreatic disorder in the Caucasian white population.
US: parenchymal atrophy with increased echogenicity, calcifications, ductal dilatation, irregular pancreatic outline, and pseudocysts.
CT: intraductal calcifications that may be scattered or clustered, focal or diffuse, have parenchymal atrophy, and have both main pancreatic and biliary ductal dilatation.
MR: decreased signal intensity on T1-weighted images, decreased heterogeneous enhancement on postgadolinium images, atrophy of the gland, and irregular dilatation of the pancreatic duct.
Chronic inflammatory process with irreversible exocrine and endocrine dysfunction. Hereditary pancreatitis is the most frequent cause of chronic pancreatitis in children.
Familial hereditary pancreatitis
Autosomal dominant disorder with variable penetrance.
Usually by 11 y of age. There is a long-term risk present for pancreatic cancer (20%).
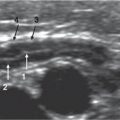
Fig. 2.28 Cystic fibrosis. Sonogram shows an echogenic pancreas of reduced thickness.Fig. 2.29 Chronic pancreatitis. Transverse sonogram through the pancreas demonstrates a small, hyperechoic pancreas and dilatation of the main pancreatic duct (between calipers: 1 = 14.5 mm).Fig. 2.30a, b Chronic pancreatitis. (a) CT shows multiple calcifications in the pancreatic body and tail (arrow). (b) Axial T2-weighted half-Fourier acquisition single-shot turbo spin echo (HASTE) MRI shows a dilated main pancreatic duct and side branches (arrows) and a calculus in the pancreatic duct (arrowhead).
Only gold members can continue reading. Log In or Register to continue