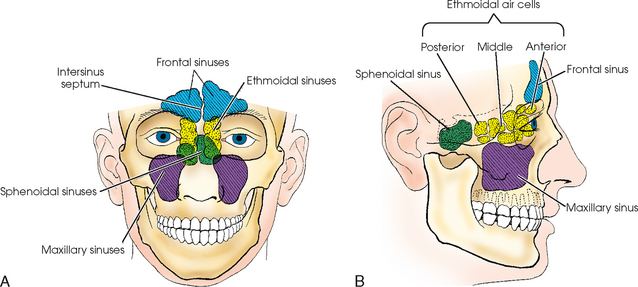
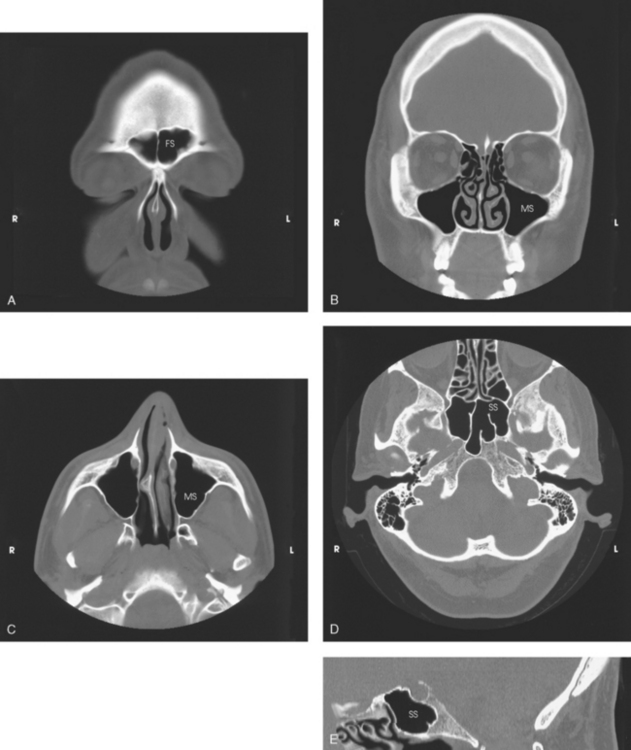
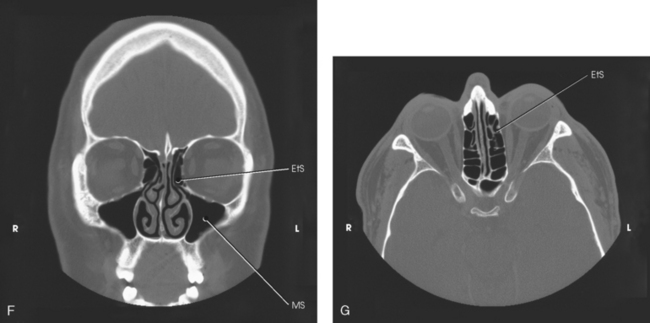
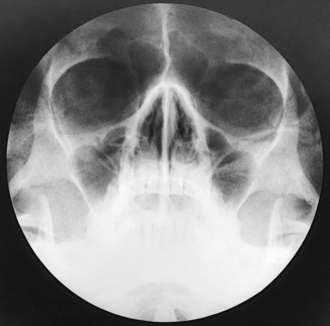
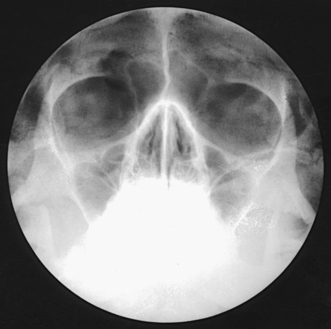
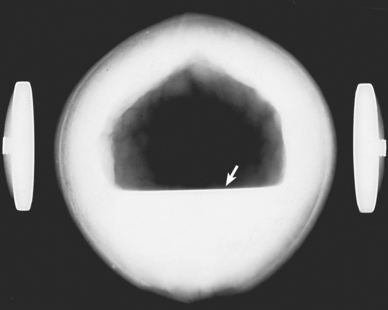
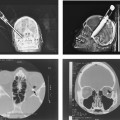
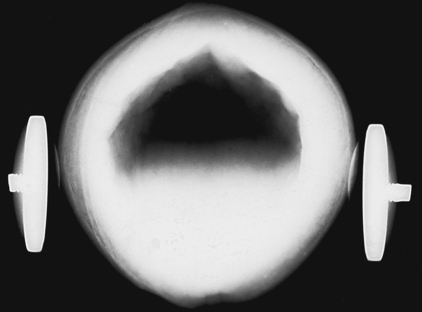
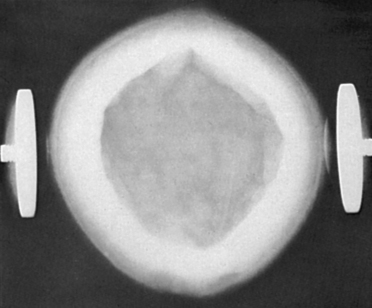
22 The air-containing cavities situated in the frontal, ethmoidal, and sphenoidal bones of the cranium and the maxillary bones of the face are called the paranasal sinuses because of their formation from the nasal mucosa and their continued communication with the nasal fossae (Figs. 22-1 and 22-2). Although the functions of the sinuses are not agreed on by all anatomists, these cavities are believed to do the following: • Serve as a resonating chamber for the voice • Decrease the weight of the skull by containing air • Help warm and moisten inhaled air • Act as shock absorbers in trauma (as airbags do in automobiles) An understanding of the actual size, shape, and position of the sinuses within the skull is made possible by studying the sinuses on computed tomography (CT) head images (see Fig. 22-2). The largest sinuses, the maxillary sinuses, are paired and are located in the body of each maxilla (see Figs. 22-1 and 22-2). Although the maxillary sinuses appear rectangular in the lateral image, they are approximately pyramidal in shape and have only three walls. The apices are directed inferiorly and laterally. The two maxillary sinuses vary considerably in size and shape but are usually symmetric. In adults, each maxillary sinus is approximately 1½ inches (3.5 cm) high and 1 to 1⅓ inches (2.5 to 3 cm) wide. The sinus is often divided into subcompartments by partial septa, and occasionally it is divided into two sinuses by a complete septum. The sinus floor presents several elevations that correspond to the roots of the subjacent teeth. The maxillary sinuses communicate with the middle nasal meatus at the superior aspect of the sinus. The frontal sinuses, the second largest sinuses, are paired and are normally located between the tables of the vertical plate of the frontal bone (see Figs. 22-1 and 22-2). The frontal sinuses vary greatly in size and form. Occasionally they are absent. One or both may be approximately ¾ to 1 inch (2 to 2.5 cm) in the vertical or lateral dimension. The sinuses often extend beyond the frontal region of the bone, most frequently into the orbital plates. The intersinus septum is usually deviated from the midline; for this reason, the frontal sinuses are rarely symmetric. Multiple septa are sometimes present. Similar to maxillary sinuses, the frontal sinuses drain into the middle nasal meatus. The two ethmoidal sinuses are located within the lateral masses of the labyrinths of the ethmoid bone. They are composed of a varying number of air cells that are divided into three main groups: anterior, middle, and posterior (see Figs. 22-1 and 22-2). The anterior and middle ethmoidal cells range in number from two to eight, and each group opens into the middle nasal meatus. The posterior cells range in number from two to six or more and drain into the superior nasal meatus. The sphenoidal sinuses are normally paired and occupy the body of the sphenoid bone (see Figs. 22-1 and 22-2). Anatomists state that often only one sphenoidal sinus is present; however, more than two sphenoidal sinuses are never present. The sphenoidal sinuses vary considerably in size and shape and are usually asymmetric. They lie immediately below the sella turcica and extend between the dorsum sellae and the posterior ethmoidal air cells. The sphenoidal sinuses open into the sphenoethmoidal recess of the nasal cavity. Radiographic density is probably more critical and more misleading in the sinuses than in any other region of the body (Figs. 22-3 to 22-5). Overpenetration of the sinuses diminishes or completely obliterates existing pathologic conditions, and underpenetration can simulate pathologic conditions that do not exist. Fig. 22-4 Overexposed radiograph of sinuses showing two artifacts caused by dirt on screens (arrows). Whenever possible, radiographs of the paranasal sinuses should be made with the patient in the upright position. This position is best for showing the presence or absence of fluid and differentiating between fluid and other pathologic conditions. The value of the upright position in sinus examinations was pointed out by Cross1 and Flecker.2 Unless sinus radiographs are almost perfect technically, they are of little diagnostic value. For this reason, a precise technical procedure is necessary in radiography of the paranasal sinuses. The first requirements are a small focal spot and clean imaging screens that have perfect contact. The radiographic contrast must similarly distinguish the sinuses from the surrounding structures. The head must be carefully positioned and rigidly immobilized, and respiration must be suspended for the exposures. The effect of body position and central ray angulation is shown in radiographs of a coconut held in position by head clamps. Fig. 22-6 shows a sharply defined air-fluid level. This coconut was placed in the vertical position, and the central ray was directed horizontally. Fig. 22-7 was also taken with the coconut in the vertical position, but the central ray was directed upward at an angle of 45 degrees to show the gradual fading of the fluid line when the central ray is not horizontal. This effect is much more pronounced in actual practice because of structural irregularities. Fig. 22-8 was made with the coconut in the horizontal position and the central ray directed vertically. The resultant radiograph shows a homogeneous density throughout the cavity of the coconut, with no evidence of an air-fluid level. Fig. 22-7 Coconut, vertical position: central ray angled 45 degrees upward. Air-fluid level is not as sharp. Fig. 22-8 Coconut, horizontal position: vertical central ray. There is no evidence of air-fluid level.
PARANASAL SINUSES

Sinuses
Maxillary Sinuses
Frontal Sinuses
Ethmoidal Sinuses
Sphenoidal Sinuses
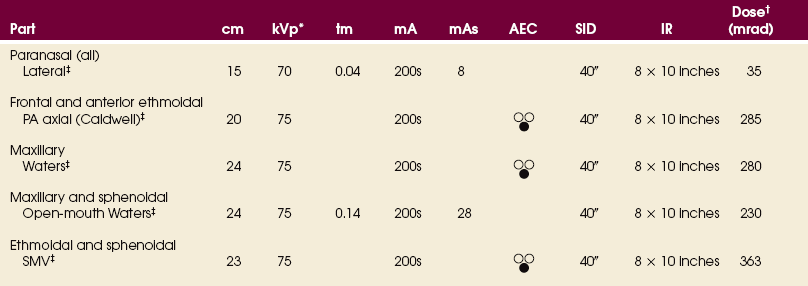
Technical Considerations

![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Radiology Key
Fastest Radiology Insight Engine