and Zdeněk Fryšák1
(1)
Department of Internal Medicine III – Nephrology, Rheumatology and Endocrinology, Faculty of Medicine and Dentistry, Palacky University Olomouc and University Hospital Olomouc, Olomouc, Czech Republic
Keywords
Parathyroid adenomaParathyroid carcinomaParathyroid cystEctopic parathyroid adenoma22.1 Essential Facts
Primary hyperparathyroidism (pHPT) is the third most common endocrine disease and the frequency of its detection gradually increases. According to data from 2009, worldwide prevalence ranges from 0.1 to 0.7% [1].
Asymptomatic cases of pHPT prevail at present. It is defined by moderately elevated serum calcium levels (s-Ca), often borderline or slightly elevated levels of serum parathyroid hormone (s-PTH), and lack of clinical symptoms. A 10-year follow-up (without specific pharmacotherapy) showed that 25% of patients developed overt disease and fulfilled the indication criteria for parathyroidectomy. In the rest of the patients, the laboratory values and bone mineral density remained unchanged [2].
In the United States and many other developed countries, for the last 30 years, asymptomatic form represents up to three-fourth of all diagnosed pHPT cases. The ratio of men to women is 3:1, with maximal incidence at the age of 50–60 years [2].
Eighty percent of pHPT cases are caused by a solitary parathyroid adenoma (PAd), 2–4% are caused by multiple parathyroid adenomas, 15% are caused by hyperplasia of all the four parathyroid glands, and about 0.5% of cases are caused by parathyroid carcinoma (PCa) [2].
Contrary to Pad, clinical signs and laboratory findings of PCa are usually severe and impressive. In PCa, s-PTH levels are three to ten times higher than normal, in contrast to the average twofold increase seen in PAd. As for serum calcium levels, these often range from 3.5 to 3.75 mmol/L in PCa, but are not that high in PAd, usually increasing by only 0.25–0.5 mmol/L above the normal [3].
In various studies the most portable and less invasive US imaging has a sensitivity of 56–100% and specificity of 40–99% in accurate localization of the PAd. 99mTc-MIBI SPECT/CT shows sensitivity of 56–100% and specificity of 83–99%. In a study by Noda, US scan, 99mTc-MIBI planar scan, and 99mTc-MIBI SPECT/CT showed accurate localization in 77.0% (47/61), 75.4% (46/61) and 88.5% (46/52) of the evaluable cases, respectively. Combination of US and 99mTc-MIBI SPECT/CT certainly contributes to the preoperative planning by indicating correct localization of single PAd [4].
Use of preoperative imaging is advantageous for identifying parathyroid lesions in ectopic locations. In those cases sensitivity of US scan was reported as 22.2%, and that of 99mTc-MIBI SPECT/CT 100% [4].
Preoperative localization of an abnormal parathyroid gland was successfully performed with US in 83.7%, with MIBI in 67.3%, with SPECT in 72.4%, while MRI in only 61.2%.
Sensitivity, specificity, and diagnostic accuracy values were 87.2%, 25.0%, and 83.0%; 70.2%, 50.0%, and 69.4%; 75.5%, 50.0%, and 74.5%; 63.8%, 50.0%, and 63.3% for US, MIBI, SPECT, and MRI, respectively [5].
Combining US and MIBI as imaging methods for preoperative imaging of pHPT often provides more satisfactory results. While the accuracy of US is relatively low in the ectopic localizations, the size of the lesion can be an important factor in the accuracy achieved with MIBI. The respective values for sensitivity, specificity, and diagnostic accuracy were 94.9%, 25.0%, and 91.1% when US was combined with MIBI [5].
Ectopic parathyroid glands (Fig. 22.9cc) result from aberrant migration during the early stages of embryonic development and lack of their successful identification may lead to lack of success in parathyroid surgery. They represent a common source of persistent or recurrent hyperparathyroidism, when missed at initial diagnosis. Their prevalence is about 2–43% in anatomical series and up to 16% and 14% in patients with primary and secondary hyperparathyroidism, respectively. Ectopic inferior parathyroids are most frequently found in the anterior mediastinum, in association with the thymus or the thyroid gland, while the most common position for ectopic superior parathyroids is the tracheoesophageal groove and retroesophageal region [6].
In current large series of 656 patients, incidence of ectopic PAd was 1.4%, which is lower than in previously reported. Eleven patients showed ectopic uptake suspicious of PAd on 99mTc-MIBI. CT confirmed diagnosis of ectopic PAd in seven patients and MRI showed PAd in two patients. Surgical and histopathological findings confirmed diagnosis of ectopic PAd in nine patients. Sensitivity and specificity of US were 11% and 100%, respectively. 99mTc-MIBI had sensitivity, specificity, positive and negative predictive values of 100%, 86%, 98% and 65%, respectively. Combination of 99mTc-MIBI with CT or MRI yielded the correct diagnosis in all cases, giving a sensitivity and specificity of 100% [7].
Of a series of 231 patients operated on for pHPT, 37 (16%) had ectopic PAd. Ectopic inferior PAds were 23 (62%): intrathymic, 7 (30%); anterosuperior mediastinal, 5 (22%); intrathyroidal, 5 (22%); within thyrothymic ligament, 4 (17%); and submandibular, 2 (9%). Ectopic superior PAds were 14 (38%): in the tracheoesophageal groove, 6 (43%); retroesophageal, 3 (22%); posterosuperior mediastinal, 2 (14%); intrathyroidal, 1 (7%); in the carotid sheath, 1 (7%); and paraesophageal. 1 (7%). 99mTc-MIBI scans were true-positive in 81%, identifying 13 of 16 retrosternal glands, and false-negative in 19%. A 16% incidence of ectopic PAd and a 100% positive predictive value of sestamibi scintigraphy underscore the importance of sestamibi imaging in patients with pHPT [8].
Presence of supernumerary parathyroid gland in the autopsy series is 5%, and presence of more than five glands is 1.25%. In the pHPT series, cases related to supernumerary parathyroid glands are rare, reported at about 0.7%. About 60% of supernumerary parathyroid glands are located in the mediastinum, the majority in thymus [9].
22.2 US Features of Parathyroids
Localizations of normal parathyroid glands [10]:
Parathyroid glands are located on the posterior face of the thyroid lobes, in extra capsular position.
There are four glands, two on each side.
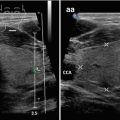
Superior parathyroid glands are located at the level of the superior third to half of the lobes (Fig. 22.1aa).
Inferior parathyroid glands are located at the inferior poles of the lobes (Fig. 22.1cc).


Fig. 22.1
(aa) Normal right superior parathyroid gland (marks) just behind the middle of RL, well shown in longitudinal section: lentil-like shape; small size 6 × 3 mm; homogeneous structure; isoechoic with thyroid gland. (bb) Normal right superior parathyroid gland (marks), CFDS: hilar vascularity; longitudinal. (cc) Normal right inferior parathyroid gland (marks) just behind the lower pole of RL, well shown in longitudinal section: lentil-like shape; small size 5 × 3 mm; homogeneous structure; isoechoic with thyroid gland. (dd) Normal right inferior parathyroid gland (marks), CFDS: hilar vascularity; longitudinal
US findings typical for parathyroid adenoma (Fig. 22.2aa) [11]:


Fig. 22.2
(aa) A 63-year-old woman with asymptomatic pHPT, laboratory: mild hypercalcemia, s-Ca 2.6 mmol/L (normal: 2.15–2.55), mild elevation of parathyroid hormone, s-PTH 82 ng/L (normal: 12–65). Small right superior parathyroid adenoma—PAd (arrows), size 15 × 11 × 5 mm and volume 0.4 mL: bean-like shape; slightly inhomogeneous; hypoechoic; normal thyroid gland; transverse. (bb) Detail of superior PAd (arrows), CFDS: flat central vascularity; transverse. (cc) Detail of superior PAd (arrows): located behind the middle of the right thyroid lobe; bean-like shaped; longitudinal. (dd) Detail of superior PAd (arrows), CFDS: flat central vascularity; longitudinal


Fig. 22.3
(aa) A 50-year-old woman with asymptomatic pHPT, laboratory: mild hypercalcemia, s-Ca 2.67 mmol/L (normal: 2.15–2.55), moderate elevation of parathyroid hormone, s-PTH 103 ng/L (normal: 12–65). Small right inferior parathyroid adenoma—PAd (arrows), size 12 × 8 × 7 mm and volume 0.4 mL: elliptical shape; homogeneous; hypoechoic; thyroid gland—Hashimoto’s thyroiditis; Tvol 14 mL, RL 7 mL, and LL 7 mL; transverse. (bb) Detail of small inferior PAd (arrows), CFDS: flat hilar vascularity; transverse. (cc) Detail of tiny inferior PAd (arrows): elliptical shape; longitudinal. (dd) Detail of small inferior PAd (arrows), CFDS: flat hilar and peripheral vascularity; longitudinal


Fig. 22.4
(aa) A 43-year-old man with asymptomatic pHPT, laboratory: moderate hypercalcemia, s-Ca 3.04 mmol/L (normal: 2.15–2.55), high elevation of parathyroid hormone, s-PTH 255 ng/L (normal: 12–65). Personal history: 20 years post total thyroidectomy for papillary thyroid carcinoma. Small left parathyroid adenoma—PAd (arrows), size 15 × 8 × 5 mm and volume 0.4 mL, confirmed by 99mTc-MIBI, as a suspicious lesion in the left thyroid bed: bean-like shape; homogeneous structure; markedly hypoechoic; transverse. (bb) Detail of the left PAd (arrows), CFDS: increased peripheral vascularity; transverse. (cc) Detail of the left PAd (arrows): elliptical shape; longitudinal. (dd) Detail of the left PAd (arrows), CFDS: focally increased peripheral vascularity; longitudinal

Fig. 22.5
(aa) A 75-year-old woman with pHPT, laboratory: moderate hypercalcemia, s-Ca 2.86 mmol/L (normal: 2.15–2.55), moderate elevation of parathyroid hormone, s-PTH 110 ng/L (normal: 12–65). Personal history: severe osteoporosis. Small left inferior parathyroid adenoma (PAd), size 15 × 14 × 7 mm and volume 0.7 mL directed towards the prevertebral space, overall US view: elliptical; inhomogeneous; hypoechoic; transverse. (bb) Detail of small inferior PAd: bean-like shaped; directed back towards the prevertebral space; transverse. (cc) Detail of small inferior PAd: bean-like shaped; directed back towards the prevertebral space; longitudinal


Fig. 22.6
(aa) A 10-year-old boy with pHPT, laboratory: severe hypercalcemia, s-Ca 2.86 mmol/L (normal: 2.15–2.55), moderate elevation of parathyroid hormone, s-PTH 110 ng/L (normal: 12–65). Personal history: nephrocalcinosis and growth retardation. Small elongated left superior parathyroid adenoma—PAd (arrows), size 12 × 5 × 4 mm and volume 0.2 mL: lentil-like shape; homogeneous structure; hypoechoic; small thyroid gland—homogeneous structure, isoechoic, Tvol 4 mL; transverse. (bb) Overall view of thyroid gland and small elongated left superior PAd (arrows), CFDS: diffusely increased vascularity; thyroid gland—normal vascularity, pattern I; transverse. (cc) Detail of small elongated left superior PAd (arrows): lentil-like shape; homogeneous structure; hypoechoic; transverse. (dd) Detail of small elongated left superior PAd (arrows): markedly elongated hypoechoic PAd along posterior wall of the upper part of LL; longitudinal. (ee) Detail of small elongated left superior PAd (arrows), CFDS: diffusely increased vascularity; longitudinalRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree