8 Facial Topography
Topography describes the positional relationship of anatomical structures. Standard textbooks of cranial topography prior to the era of cross-sectional imaging favored the depiction of anatomic structures as conceived from dissected specimens, thereby drawing on the vast experience of surgical specialties.
Progress made in cross-sectional imaging methods requires a special 3D knowledge of anatomic structures for interpretation of parallel sections. Equidistant serial CT and MR images of the head may be likened to an architect’s rendition of an entire building and its different floors. While right-angled objects predominate in architecture, anatomical structures have more complicated shapes and result in variable patterns.
The position of the individual slice is of special importance in anatomy. This may be seen in ▶Fig. 3.1 for the coronal series in lateral view, ▶Fig. 4.1a and ▶Fig. 4.1b for the sagittal series in frontal view, and ▶Fig. 5.1, ▶Fig. 5.16, and ▶Fig. 6.3 for the biccomissural, supraorbito-suboccipital, and the brainstem series in lateral view, respectively. The coronal series (see ▶Fig. 3.2 up to ▶Fig. 3.25) corresponds to an anterior view. Therefore, the anterior line of a slice determines sectioned structures within the slice (see ▶Fig. 3.1). Anatomical structures lie in the intervals between adjacent lines; MR images were selected according to the schematic representation. The sagittal series has been depicted from the medial aspect (see ▶Fig. 4.2 to ▶Fig. 4.13). The bicommissural and supraorbito-suboccipital series (see ▶Fig. 5.2 to ▶Fig. 5.30) as well as the brainstem series (see ▶Fig. 6.4 to ▶Fig. 6.13) have been viewed from below. Therefore, the line below each encircled digit determines sectioned structures within the slice (see ▶Fig. 5.1, ▶Fig. 5.16, and ▶Fig. 6.3).
8.1 Facial Bones
The facial skeleton or the viscerocranium forms the bony confines for the proximal ends of the respiratory and digestive systems and encloses the orbital cavity. The nasal skeleton is composed of five bones, while the jaw is composed of four. Individual bones may form part of two or more regions due to their proximity to each other. The hard palate thus forms the floor of the nasal cavity as well as the roof of the oral cavity.
8.1.1 Bones of the Nasal Skeleton
The ethmoid develops as an unpaired bone in the cartilaginous nasal capsule, and is composed of a central T-piece and paired lateral parts as seen on coronal sections:
Cribriform plate (lamina cribrosa; see ▶Fig. 3.3c, ▶Fig. 3.17, and ▶Fig. 4.8): forms the horizontal limb of the “T.”
Perpendicular plate: corresponds to the vertical limb of the “T.”
Ethmoid cells (see ▶Fig. 3.1b, ▶Fig. 3.2a, ▶Fig. 3.2b, ▶Fig. 3.16, ▶Fig. 4.1b, ▶Fig. 4.3a, ▶Fig. 4.3b, ▶Fig. 4.9, ▶Fig. 5.1b, ▶Fig. 5.4, ▶Fig. 5.17, ▶Fig. 5.35, and ▶Fig. 6.9a): these lie between the nasal and orbital cavities and inferior to the anterior cranial fossa.
The cribriform plate inserts into the frontal bone as a median and paramedian structure. This thin bony plate exhibits several perforations traversed by olfactory nerves, which pass from the olfactory mucosa to the olfactory bulb in the olfactory fossa.
Clinical Notes
The depth of the olfactory fossa from the roof of the ethmoid is relevant to the planning of a surgical procedure on the ethmoid cells.
This is divided into three types in accordance with Keros classification:
Keros Type I: 1–3 mm
Keros Type II: 4–7 mm
Keros Type III: 8–16 mm (also termed the “dangerous ethmoid”)189 , 289
The crista galli protrudes into the cranial cavity from the ethmoidal plate in the median plane (see ▶Fig. 3.2c, ▶Fig. 3.2d, ▶Fig. 3.16, ▶Fig. 4.1b, ▶Fig. 4.2c, ▶Fig. 4.2d, ▶Fig. 4.8, ▶Fig. 5.6a, ▶Fig. 5.6b, ▶Fig. 5.18, ▶Fig. 6.12a, and ▶Fig. 6.13a). The falx cerebri is attached to this bony process.
The perpendicular plate is a continuation of the crista galli below the cribriform plate and forms the upper part of the bony nasal septum. The orbital plate (previously: papyracea, see ▶Fig. 3.2c, ▶Fig. 3.2d, ▶Fig. 3.3c, ▶Fig. 3.3d, ▶Fig. 3.16, ▶Fig. 3.17, and ▶Fig. 6.10a) forms the lateral boundary of ethmoid cells, separating them from the orbital cavity. The ethmoid cells are air-containing spaces which communicate with the nasal cavity. The anterior and middle ethmoidal cells open below the middle nasal concha while the posterior ethmoidal cells open above it. The entire ethmoidal labyrinth measures approximately 10 mL in volume.336 The superior and medial nasal conchae protrude into the nasal cavity from the medial aspect of the ethmoid labyrinth. The middle canal lies below the middle concha (see ▶Fig. 3.2a, ▶Fig. 3.2b, ▶Fig. 3.3a, ▶Fig. 3.3b, ▶Fig. 3.4a, and ▶Fig. 3.4b). The anterior and middle ethmoid cells as well as the maxillary and frontal sinuses drain into a crescent shaped opening in the middle canal, the hiatus semilunaris (see ▶Fig. 3.2a, ▶Fig. 3.3a, ▶Fig. 4.3a, ▶Fig. 6.8a, and ▶Fig. 6.9a). This drainage area together with the middle canal is also known as the “ostiomeatal complex”.
The independent inferior nasal concha with a length of about 4 cm is larger than the other conchae. This hook shaped structure seen above the palate on coronal sections forms a landmark for imaging (see ▶Fig. 3.2a, ▶Fig. 3.2b, ▶Fig. 3.3a, ▶Fig. 3.3b, ▶Fig. 3.4a, ▶Fig. 3.4b, ▶Fig. 3.16, ▶Fig. 3.17, ▶Fig. 4.3a, ▶Fig. 4.3b, ▶Fig. 5.3, ▶Fig. 6.4a, and ▶Fig. 6.5a).
The lower part of the bony nasal septum is formed by the vomer, an unpaired bone. The nasal septum is composed of a cartilaginous component in addition to its two bony parts.
The paired nasal bones are small oblong bones forming the upper part of the nasal bridge.
The small, four-sided, and paired lacrimal bones lie within the medial wall of the orbit, forming part of the lateral nasal wall.
8.1.2 Skeletal Anatomy of the Jaw
The maxilla is the central bone of the face, abutting the orbital, nasal, and oral cavities and forming most of the hard palate. It comprises of a central piece or body and three processes:
The maxillary sinus occupies the large body of the maxilla and is visualized as the largest pneumatized paranasal sinus in coronal (see ▶Fig. 3.1b, ▶Fig. 3.2a, ▶Fig. 3.2b, ▶Fig. 3.3a, ▶Fig. 3.3b, ▶Fig. 3.4a, ▶Fig. 3.4b, and ▶Fig. 3.17), sagittal (see ▶Fig. 4.1b, ▶Fig. 4.4a, ▶Fig. 4.4b, ▶Fig. 4.6a, ▶Fig. 4.6b, and ▶Fig. 4.10), and axial sections (see ▶Fig. 5.1b, ▶Fig. 5.31, and ▶Fig. 6.3).
The frontal process of maxilla extends between the nasal and lacrimal bones up to the frontal bone.
The zygomatic process abuts the zygomatic bone.
The palatal process is a horizontal bony plate which abuts the palatine bone at its posterior aspect, both of these forming the hard palate (see ▶Fig. 3.1b, ▶Fig. 3.2c, ▶Fig. 3.2d, ▶Fig. 3.3c, ▶Fig. 3.3d, ▶Fig. 3.4c, ▶Fig. 3.4d, ▶Fig. 3.16, ▶Fig. 3.17, ▶Fig. 4.3c, ▶Fig. 4.3d, and ▶Fig. 4.8).
The alveolar process contains alveoli that hold the teeth of the upper jaw, which is resorbed following tooth loss, as is well seen in the maxilla on the sagittal series. The maxilla is narrow at the site where the upper teeth were located and lacks the rugged alveolar process which extends into the oral cavity (see ▶Fig. 3.3c, ▶Fig. 3.3d, ▶Fig. 4.8, ▶Fig. 4.9, and ▶Fig. 5.2).
The palatine bone is composed of the horizontal plate forming part of the hard palate and an approximately vertical plate which forms the medial boundary of the pterygopalatine fossa.
The zygomatic bone inserts between the maxilla, temporal bone, and frontal bones (see ▶Fig. 3.1b, ▶Fig. 3.2c, ▶Fig. 3.2d, ▶Fig. 3.5b, ▶Fig. 3.17, ▶Fig. 4.1b, ▶Fig. 4.7c, ▶Fig. 4.7d, ▶Fig. 5.3, ▶Fig. 5.5, ▶Fig. 5.17, ▶Fig. 5.31, and ▶Fig. 6.5a).
The lower jaw or mandible is the only mobile facial bone which articulates with the base of the skull. The anterior part or body resembles a bent horseshoe (see ▶Fig. 3.1b, ▶Fig. 3.2c, ▶Fig. 3.2d, ▶Fig. 3.3c, ▶Fig. 3.3d, ▶Fig. 3.16, ▶Fig. 4.1b, ▶Fig. 4.2c, ▶Fig. 4.2d, ▶Fig. 4.4c, ▶Fig. 4.4d, and ▶Fig. 4.8), while the ramus of the mandible projects upwards from the body (see ▶Fig. 3.1b, ▶Fig. 3.5c, ▶Fig. 3.5d, ▶Fig. 3.6c, ▶Fig. 3.6d, ▶Fig. 3.20, ▶Fig. 4.1b, ▶Fig. 4.7c, and ▶Fig. 4.12). The teeth of the lower jaw are contained within the alveoli of the body of mandible. The alveolar part undergoes resorption following loss of teeth, such that the mandibular canal comes to lie closer to the toothless alveolar margin (see ▶Fig. 3.16 and ▶Fig. 3.18). Running upward from the body at the angle of the mandible, the ramus of the mandible then divides into two processes, the pointed coronoid process (anterior, see ▶Fig. 3.1b and ▶Fig. 4.13) and the condylar process (posterior, see ▶Fig. 4.13). The coronoid process may be considered to represent an ossified tendon as it lies buried within the tendinous fibers of the temporalis (see ▶Fig. 4.7c). The condylar process first tapers to the neck of the mandible (see ▶Fig. 3.1b and ▶Fig. 3.21), extending superiorly to the transversely positioned head of mandible (see ▶Fig. 3.1b, Fig. 3.7c, ▶Fig. 3.7d, and ▶Fig. 3.21). The mandibular foramen lies on the inner aspect of the ramus, through which the inferior alveolar nerve and vessels enter the mandibular canal (see ▶Fig. 4.7a, ▶Fig. 4.7c, and ▶Fig. 4.12). Complex spatial relationships of pathological changes involving the facial skeleton (fractures, destructions) are well illustrated with high-resolution spiral CT techniques or modern volume tomographs (e.g., dental volume tomography) using thin slices.365 Axial and reformatted coronal and sagittal sections are employed during CT examinations. Axial images are preferably obtained by sectioning parallel to the infraorbitomeatal plane,254 , 365 with a wide window being used to image bony structures and a narrow window for soft tissues.
8.2 Nasal Cavity and Paranasal Sinuses
8.2.1 Topography
The paired nasal cavities extend from the nostrils and continue via the vestibule into the nasal cavity proper, which in turn opens into the nasopharynx at the posterior nasal openings or choanae. The nasal cavity is divided by the nasal septum into right and left halves.
All paranasal sinuses are connected to the nasal cavity and are composed of the following:
Ethmoid air cells
Maxillary sinus
Sphenoid sinus
Frontal sinus
The centrally positioned nasal cavity and paranasal sinuses, extending above and below Reid’s baseline, are well seen on coronal and sagittal sections (see ▶Fig. 3.2 to ▶Fig. 3.25 and ▶Fig. 4.2 to ▶Fig. 4.13). The sphenoid sinus may extend almost up to the meatovertical line posteriorly. The nasal cavities and paranasal sinuses lie inferior to the anterior cranial fossa, inferomedial to the orbits and the middle cranial fossa, and superior to the oral cavity. Posteriorly, the nasal cavity continues into the pharynx through the choanae between the fourth and fifth coronal sections. The sphenoid sinus (see ▶Fig. 3.6a and ▶Fig. 3.6b) is seen lying above the pharynx (see ▶Fig. 3.6a and ▶Fig. 3.6b) in the fifth coronal section. These regions exhibit great interindividual variability. The paranasal sinuses are of clinical importance since they may be involved by infectious processes, tumors, and trauma. Ultrasound, CT, MRI, and endoscopy are all useful diagnostic methods in the evaluation of such lesions.
The medial wall of the nasal cavity is formed by the nasal septum (see ▶Fig. 3.2a, ▶Fig. 3.2b, ▶Fig. 3.3a, ▶Fig. 3.3b, ▶Fig. 3.16, ▶Fig. 4.1b, ▶Fig. 4.2b, ▶Fig. 4.8, ▶Fig. 5.3, ▶Fig. 5.31, and ▶Fig. 6.6a), which lies nearly in the midline, and may be laterally deviated in its anterior or posterior parts. This is termed “septal deviation” (see ▶Fig. 3.3a, ▶Fig. 3.3b, and ▶Fig. 3.17).
The lateral wall of the nasal cavity is enlarged by medially projecting conchae, each roofing a canal:
The superior nasal canal is short, averaging less than 2 cm in length,332 into which the posterior ethmoidal cells drain.
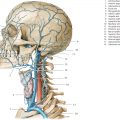
The middle nasal canal is connected to the frontal sinus, anterior, and middle ethmoidal cells, and to the maxillary sinus via the hiatus semilunaris (see ▶Fig. 3.2a, ▶Fig. 3.2b, ▶Fig. 3.3a, ▶Fig. 4.3a, and ▶Fig. 6.9a). The middle nasal concha has been partly sectioned tangentially in ▶Fig. 4.3a such that the anterior and superior parts of the semilunar hiatus (see ▶Fig. 4.3a) are visible. The postero-inferior part, which is obscured by the middle concha, has been indicated by a broken line. The nasolacrimal duct (see ▶Fig. 6.6a and ▶Fig. 8.1) drains into the inferior canal and carries tears into the nasal cavity.

Ethmoidal cells and the maxillary sinus have already been described along with their corresponding bones. The sphenoid and frontal sinuses are paired, with the paired sphenoid sinus usually lying within the body of the sphenoid. In 12% of cases the sphenoid sinus extends only as far as a perpendicular drawn through the tuberculum sellae (presellar type); it surrounds the pituitary fossa in 84% (sellar type); and is located outside the body of the sphenoid in 4%.332 A sphenoid sinus of the sellar type is seen in the coronal series (see ▶Fig. 3.1b, ▶Fig. 3.5a, ▶Fig. 3.5b, ▶Fig. 3.6a, ▶Fig. 3.6b, ▶Fig. 3.7a, ▶Fig. 3.7b, and ▶Fig. 3.8a). The sphenoid sinus drains into the sphenoethmoidal recess above the superior concha. The septum separating both sphenoid sinuses is frequently asymmetrical (see ▶Fig. 3.5a). The roof of the sphenoid sinus is closely related to the optic nerve (see ▶Fig. 3.5a and ▶Fig. 3.5b). Familiarity with the sphenoid sinus is of special importance in the trans-sphenoid approach for surgeries on the pituitary gland (Onodi cells, sphenooptic recess). Parts of the optic canal are formed only by the sheath of the optic nerve and the mucous membrane of the sinus in four percent of cases. The optic nerve is therefore vulnerable to injury in the trans-sphenoid approach to the pituitary.332
The frontal sinus is highly variable and often asymmetrical (see ▶Fig. 4.1b). The left frontal sinus has been sectioned in the anterior part of the frontal bone on the right of the head (see ▶Fig. 4.2a and ▶Fig. 4.2b). Its anterior wall forms the bony supraciliary arch, which exhibits individual variations. The floor of the frontal sinus is separated from the orbit by a thin plate of bone.
8.2.2 Blood Supply of Paranasal Sinuses
The walls of the nasal cavity are supplied by branches of the maxillary and ophthalmic arteries. The maxillary artery (see ▶Fig. 9.1) gives off the sphenopalatine artery, which exits the pterygopalatine fossa through the sphenopalatine foramen under the nasal mucus membrane, supplying the posterior aspect of the lateral and medial walls of the nasal cavity. The anterior ethmoidal artery arises from the ophthalmic artery that enters the nasal cavity following a circuitous course through the cranium. This complicated course was probably an outcome of late phylogenetic development of an entirely bony orbital cavity, together with the marked enlargement of the neocortex in mammals. The anterior ethmoidal artery exits the orbital cavity through the anterior ethmoidal foramen and first enters the anterior cranial fossa; passing through the cribriform plate into the anterior part of the nasal cavity, it divides to supply its medial and lateral walls.
Veins arising in the nasal mucosa drain into the orbital veins, the pterygoid venous plexus and facial veins. Lymph nodes at the angle of the jaw and posterior to the pharynx receive lymphatic drainage from the nasal mucosa.
8.2.3 Nerve Supply of the Nasal Cavity
The region of the olfactory epithelium in the nasal mucus membrane may be differentiated from the ciliated respiratory epithelium as it is thicker and has a slightly brown tinge. The olfactory region is composed of four Cent-like sized fields in the center of the superior nasal concha and the corresponding area of the nasal septum opposing it. Histologically, the olfactory epithelium contains olfactory cells, the basal axons of which give rise to olfactory fibers. These fibers of the first (olfactory) cranial nerve then run through the cribriform plate of the ethmoid into the cranial cavity and terminate in the olfactory bulb.
Sensory supply of the nasal cavity is provided by the ophthalmic and maxillary nerves, the terminal branches of which carry viscerosecretory fibers to the mucous glands in the nasal mucosa.
The ophthalmic nerve gives off the nasociliary nerve, which in turn gives rise to the anterior ethmoidal nerve. This then accompanies the anterior ethmoidal artery in its circuitous course through the anterior cranial fossa to supply the anterior nasal mucosa.
Branches of the maxillary nerve supply the posterior aspect of the nasal mucosa on its medial and lateral aspects.
The greater petrosal nerve contains parasympathetic preganglionic nerve fibers to nasal mucosal glands. Postganglionic fibers from the pterygopalatine ganglion (see ▶Fig. 10.43b) join sensory fibers in the pterygopalatine fossa.
Sympathetic postganglionic nerve fibers also run alongside arterial branches to the pterygopalatine fossa and continue with sensory fibers to nasal mucosal glands.
8.3 Orbit
8.3.1 Topography
The orbit contains the globe of the eye and is the receptor organ of the visual system (see ▶Section 10.6). The eyeball is protected by the following structures77:
Bony walls of the orbit
Eyelids
Conjunctiva
Lacrimal apparatus
A fascial sheath or Tenon’s capsule surrounds the eyeball as a joint capsule might surround a sphere.
The extraocular muscles enable extremely precise movements of the eyeball.
The optic nerve courses posteriorly from the globe to the optic chiasma.
The shape of the orbital cavity resembles a hollow four-sided pyramid. Its base is directed outward with the optic canal forming its apex, at which point the optic nerve exits the orbit. The apex of the pyramid is directed posteromedially.
The four walls of the orbit are best seen in coronal sections (roof of orbit, see ▶Fig. 3.2c and ▶Fig. 3.2d; floor of orbit, see ▶Fig. 3.2c and ▶Fig. 3.2d) and appear markedly rounded posteriorly, where they merge into each other (see ▶Fig. 3.4 and ▶Fig. 3.17). The ophthalmic artery and optic nerves are closely opposed to one another within the optic canal (see ▶Fig. 3.5a, ▶Fig. 3.5b, and ▶Fig. 3.5c).
The anterior pole of the eyeball lies approximately in a plane tangential to the superior and inferior margins of the orbit. The globe is displaced in a sagittal direction by space-occupying retrobulbar processes within the orbit. Edema, hematomas, inflammatory lesions, and tumors can all push the eyeball forward if the bony walls of the orbit do not give way. Blunt compression injury, such as a blow with a fist, can result in a blow-out fracture of the thin orbital floor whereby orbital contents are forced into the maxillary sinus (see ▶Fig, 3.2a, ▶Fig. 3.2b, ▶Fig. 3.3a, and ▶Fig. 3.3b).
The orbit is connected to the following structures via several openings:
The middle cranial fossa, through the optic canal (see ▶Fig. 3.18 and ▶Fig. 5.37) for the optic nerve and the ophthalmic artery, and through the superior orbital fissure (see ▶Fig. 3.18) for the third, fourth, the first division of the Vth and the VIth cranial nerves and the superior ophthalmic vein.
The infratemporal and pterygopalatine fossae, through the inferior orbital fissure for the zygomatic nerve and inferior ophthalmic vein.
The nasal cavity, through the nasolacrimal canal for the nasolacrimal duct.
The face, through the infraorbital canal (see ▶Fig. 3.2b, ▶Fig. 3.16, and ▶Fig. 3.17) for infraorbital vessels and nerves (see ▶Fig. 3.2b, ▶Fig. 3.2d, ▶Fig. 3.3a, ▶Fig. 3.3b, ▶Fig. 3.3c, and ▶Fig. 3.3d).
The anterior cranial fossa, through the anterior ethmoidal foramen for the anterior ethmoidal vessels and nerves.
Posterior ethmoidal cells and the sphenoid sinus, through the posterior ethmoidal foramen for posterior ethmoidal vessels and nerves.
The invention of the ophthalmoscope by Hermann von Helmholtz in 1850 refined ophthalmoscopic examination of the globe which is of significance even today. High-resolution retinal examinations are furthermore possible using optic coherence tomography.659 Advances in new imaging techniques (MRI) are most evident in the diagnosis of retrobulbar pathology of the orbit; the retrobulbar space will therefore be described in greater topographic detail.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


