18 Partial and Total Anomalous Pulmonary Venous Connections
With Monica Epelman
Definition
 Abnormal connection of some or all of the pulmonary veins to a systemic vein or the right atrium (Fig. 18.1).
Abnormal connection of some or all of the pulmonary veins to a systemic vein or the right atrium (Fig. 18.1).
 Isolated or associated with other cardiac anomalies
Isolated or associated with other cardiac anomalies
 Partial and total anomalous drainage are described as two distinct entities, as the classification, pathophysiology, and diagnosis are quite different.
Partial and total anomalous drainage are described as two distinct entities, as the classification, pathophysiology, and diagnosis are quite different.
 Partial anomalous venous connection
Partial anomalous venous connection
- • Anomalous connection of one or more pulmonary veins, which may be unilateral or bilateral
- • Uncommonly mixed drainage to multiple sites with anomalous connection of more than one pulmonary vein
- • Anomalous drainage of right pulmonary veins significantly more common
- • Partial anomalous drainage of a right pulmonary vein to superior or inferior vena cava is associated with a sinus venosus atrial septal defect.
- • Partial anomalous drainage of a right pulmonary vein to right atrium can also be associated with a secundum atrial septal defect.
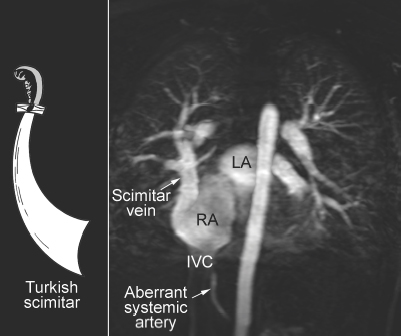
- • Partial anomalous drainage of right pulmonary veins to the inferior vena cava–right atrial junction is associated with the scimitar syndrome (hypogenetic right lung syndrome, congenital venolobar syndrome) (Fig. 18.2).
- – Hypoplasia or aplasia of one or more lobes of the right lung with lobation, segmentation, and fusion abnormalities, and hypoplasia and abnormal branching pattern of the right pulmonary artery and bronchus
- – Systemic arterial blood supply to the right lung in most cases. True pulmonary sequestration with disconnected bronchial supply is rare.
- – Occasionally with horseshoe lung or crossover lung
- – Anomalies of right hemidiaphragm
- – Anomalies of bony thorax and soft tissues with excess extrapleural areolar tissue
- • Partial anomalous drainage of a left pulmonary vein(s) is usually into the left innominate vein or coronary sinus and often associated with a secundum atrial septal defect.
- • Partial anomalous drainage is common in left isomerism.
 Total anomalous pulmonary venous connection
Total anomalous pulmonary venous connection
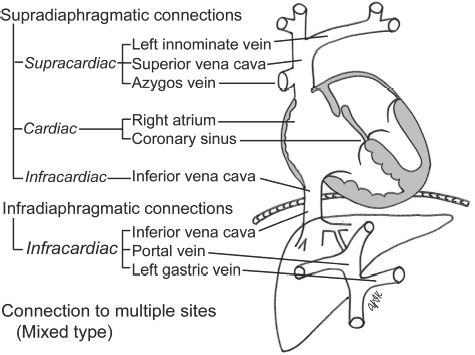
Fig. 18.1 Classification of anomalous pulmonary venous connections according to the site of abnormal connection.
Fig. 18.2 Scimitar syndrome. IVC, inferior vena cava; LA, left atrium; RA, right atrium.
Pathophysiology
 Depends on how much of the pulmonary circulation empties into the systemic circulation, presence of pulmonary venous obstruction, and associated cardiac anomalies
Depends on how much of the pulmonary circulation empties into the systemic circulation, presence of pulmonary venous obstruction, and associated cardiac anomalies
 Partial anomalous pulmonary venous connection
Partial anomalous pulmonary venous connection
- • Basically a left-to-right shunt increasing the pulmonary-to-systemic flow ratio proportional to the number of veins connected to the right-sided circulation and to the presence of an associated atrial septal defect
- • Mild physiologic abnormality with a hemodynamically relevant left-to-right shunt usually with complete return of all veins from one lung or with an associated atrial septal defect
- • Right atrium and ventricle dilate, leading to right heart volume overload.
- • Increased pulmonary blood flow rarely leads to pulmonary artery hypertension.
- Total anomalous pulmonary venous connection
- • Unobstructed pulmonary venous return causes a left-to-right shunt, and with all blood bypassing the left atrium, an obligatory interatrial right-to-left shunt is necessary for survival.
- • Complete mixing of systemic and pulmonary venous blood within the heart, resulting in identical oxygenation in all four chambers and produces cyanosis
- • Right ventricular volume overload with increased pulmonary vascularity; may lead to right heart failure
- • Left atrium and ventricle receive less than normal flow and may show some degree of underdevelopment.
- • Obstructed pulmonary venous return results in pulmonary venous and arterial hypertension, pulmonary edema, and diminished pulmonary return, leading to low cardiac output.
- • Severe pulmonary venous congestion results in increased pulmonary lymphatic flow and increased flow through available alternative venous pathways.
- • Reflex pulmonary arterial vasoconstriction leads to increased pulmonary vascular resistance and decrease in pulmonary blood flow.
- • Increased right-sided pressure overload leads to right heart failure.
- • Restriction to flow may result from an obstruction of the pulmonary venous circuit or across the atrial septum.
- • Infracardiac type is almost always obstructed and is a result of a combination of factors:
- – Following closure of the ductus venosus, the pulmonary venous flow is forced through the portal sinusoid system, resulting in significant impedance of blood flow by the hepatic parenchyma.
- – Extrinsic obstruction of the descending anomalous draining vein passing through the diaphragm hiatus
- – Length of the descending anomalous draining vein
- – Stenosis at connection of anomalous vein with portal vein
- • Supracardiac type, seldom obstructed
- – Intrinsic stenosis at connection of common pulmonary vein with vertical vein or its attachment to the innominate vein
- – Extrinsic obstruction as vertical vein passes through a triangular space between left pulmonary artery, left ductus arteriosus, and left main bronchus, called anatomical vice
- – Intrinsic stenosis of vertical vein
- • Cardiac type, rarely obstructed
- – Stenosis at connection of common vein to coronary sinus