Overview
Anatomy and Physiology
• See Chapter 22, Adult Echocardiography Scanning Protocol.
Sonographic Appearance
• The pericardium is the brightest structure and appears almost white.
• The valves tend to be the next brightest, appearing light gray to almost white depending upon how perpendicular the valve is to the ultrasound beam.
• The myocardium has a homogeneous texture and appears gray.
• The area within the chambers, vessels, and any fluid appear anechoic.
Preparation
Patient Prep
• ECG leads should be attached to the right shoulder, left shoulder, and left hip regions.
Transducer
• 7.5 MHz used for premature infants.
• 5.0 MHz to 7.5 MHz used for neonates to infants.
• 5.0 MHz to 3.5 MHz for toddlers (depending on the body surface area).
• 3.5 MHz to 2.5 MHz used for children and teenagers (depending on body habitus).
Patient Position
• Neonates and infants may remain supine.
• Children (classified as anyone under the age of 17 years) should be in the left lateral decubitus position.
Breathing Techniques
• Normal respiration.
Transducer Orientation
• Images are obtained from the following 4 windows:
1. Parasternal
2. Apical
3. Subcostal
4. Suprasternal
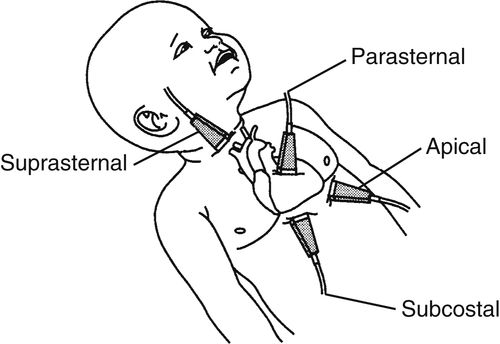
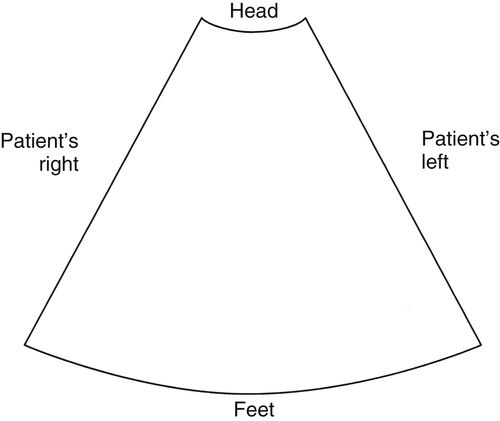
• Scanning is performed in the anatomically corrected position; therefore, the sector is inverted for the subcostal and apical views. The study thus provides an anatomic reference for the surgeon.
• The ECG rate is increased to 100% for neonates because of the higher infant heart rate. This allows for easier interpretation of the Doppler and ECG.
Pediatric Heart Survey
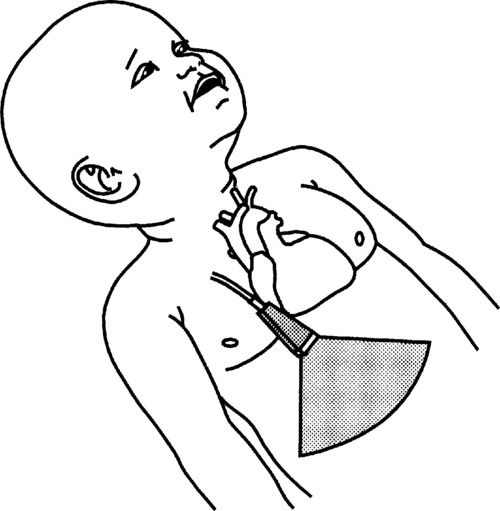
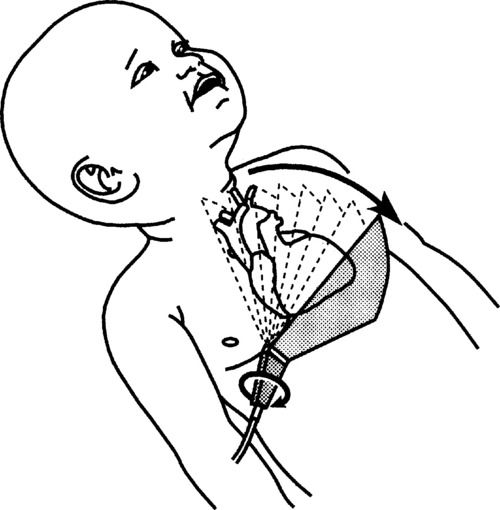
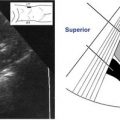
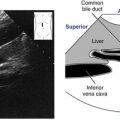
1. Begin by placing the transducer midline on the abdomen, below the xiphoid process. Flip the sector, so the point appears at the bottom of the screen. Looking at the monitor, the image should be oriented so the structures on the patient’s left appear to the right of the screen. Point directly anterior to posterior, visualizing the liver and cross sections of the inferior vena cava (IVC) (found on the patient’s right) and aorta (to the patient’s left). This establishes normal situs of the abdominal structures.
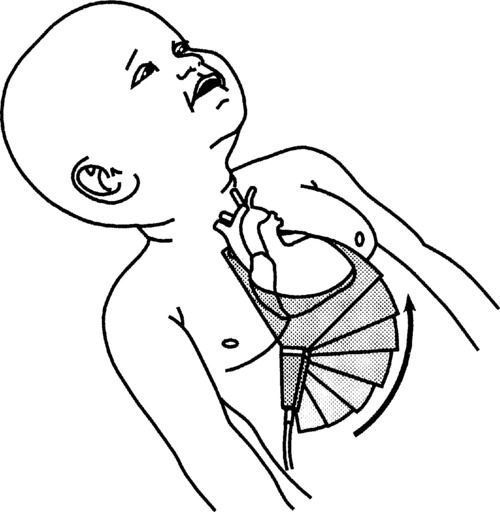
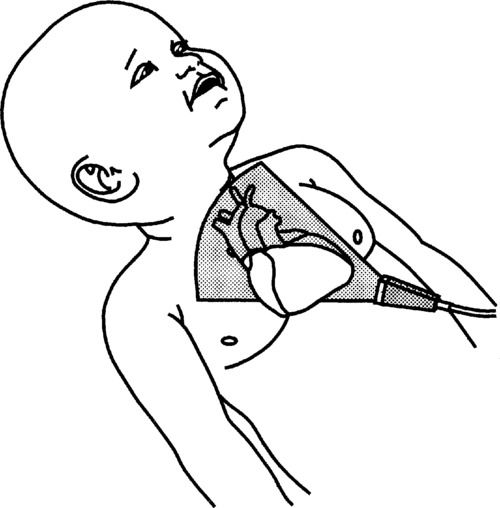
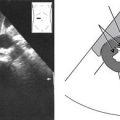
2. Slowly angle superiorly, demonstrating the entry of the hepatic veins into the IVC and eventually the IVC into the right atrium (RA). Continue to angle superiorly until the 4 chambers of the heart are observed. Verify the orientation of the heart, its chambers, and valves. The apex should appear to the right of the screen. Look for the 4 pulmonary veins to enter the left atrium (LA). Use color Doppler and pulsed-wave (PW) Doppler to assess the flow across the mitral (MV) and tricuspid (TV) valves. Use color Doppler for the interatrial septum and interventricular septums to assess for the presence of a shunt. Pulse any turbulence observed. Use continuous-wave (CW) Doppler to evaluate any high velocities (e.g., ventricular septal defect, tricuspid regurgitation).
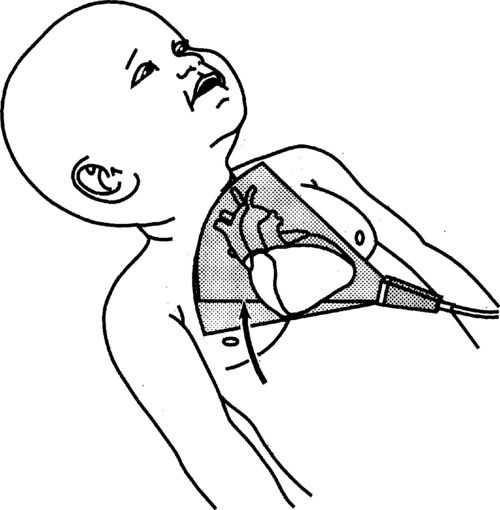
3. Continue to angle the transducer more superiorly, opening the left ventricular outflow tract (LVOT) and the aorta. Use color and PW Doppler for these, looking for the presence of regurgitation or turbulence.
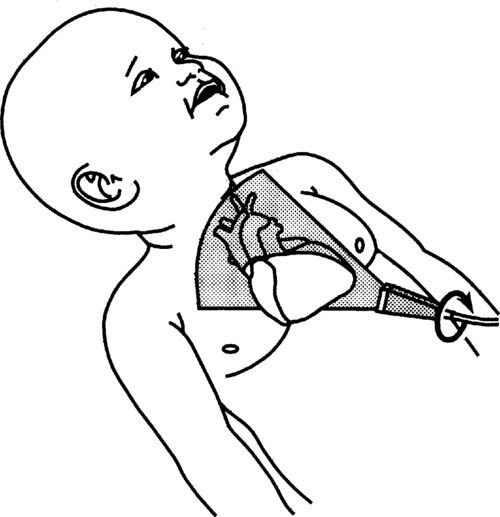
4. Tilting the transducer even more superiorly will open the right ventricular outflow region, pulmonic valve (PV), and pulmonary artery (PA). Use color and PW Doppler to assess the PV for turbulence and for the presence of a patent ductus arteriosus (PDA).
5. Slowly tilt inferiorly to return to the 4-chamber view, then rotate the transducer clockwise 90 degrees. This is the orientation for the subcostal short axis views. Begin by directing the transducer toward the right shoulder, demonstrating the entry of the superior vena cava and inferior vena cava into the right atrium. Use color Doppler to scan the IVC and superior vena cava (SVC). Use PW to establish normal flow profiles.
6. Slowly begin to angle the transducer toward the left shoulder, first observing the interatrial septum, then the PA, PV, and aortic valve (AV). Use color Doppler and PW for any turbulence observed. Continue to sweep leftward through the mitral and tricuspid valves, assessing thickness and motion, to the cross section of the left (LV) and right (RV) ventricles. Slowly sweep beyond the papillary muscles to the apical region, all the while assessing thickness and contractility. Repeat using color Doppler, looking for any shunts.
7. Move the transducer to the left flank, directing the beam towards the right shoulder. This will dissect the heart from apex to base, and the apical 4-chamber view is visualized. The left side of the heart should appear to the right of the screen. The LA, LV, RA, and RV are observed as well as the mitral and tricuspid valves. Assess the chamber sizes and valves. Use color and PW Doppler for both the valves, and use CW Doppler for any high-velocity flow.
8. Angle the transducer slightly anterior to open the LVOT and aorta. This is the apical 5-chamber view. Use color and PW Doppler for the aortic valve and LVOT.
9. Rotate the transducer clockwise to open the outflow tract even more. This produces the apical long axis. In addition, the AV, LA, LV, and MV are seen. Again, use color Doppler for the LVOT region and PW Doppler up the IVS, looking for a step-up in velocity or any turbulence.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


