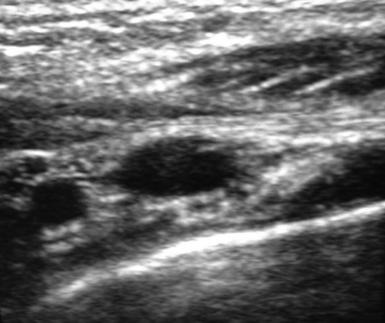
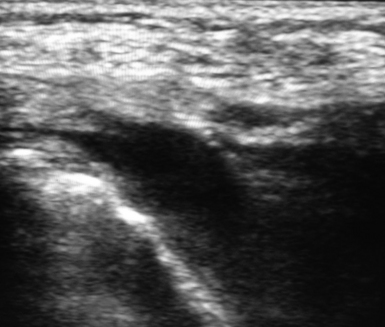
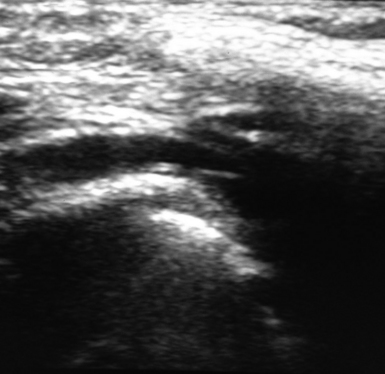
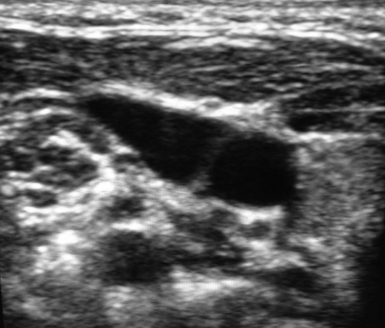
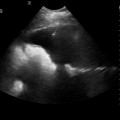
13 Ultrasound offers the advantage of preprocedural evaluation of all possible venipuncture sites as detailed in previous chapters. This is an essential feature of the ultrasound method when applied in the pediatric intensive care unit (PICU).1–4 A thorough ultrasound examination allows the identification of vessels that may be difficult to puncture (e.g., small vessel diameter, especially in relation to the size of the catheter used; vessels collapsing during breathing; vessels in close proximity to arteries or the pleura; or the presence of thrombosis, hematomas, strictures, or anatomic variations). Ideally, the external diameter of the catheter should not exceed a third of the internal diameter of the vein (e.g., a 3-Fr catheter should be inserted into a vein with an internal diameter of 3 mm [≥9 Fr = 3 mm] as measured by ultrasound, a 4-Fr catheter would require a 4-mm vein, and so on).3 In the PICU, preprocedural scanning may optimize the choice of catheter type (e.g., peripherally inserted central catheter [PICC] vs. a centrally inserted venous catheter) or puncture site (venous segments of the superior vs. the inferior vena cava network) and thus facilitate real-time ultrasound-guided catheterization of the vessel. Implementation of the holistic approach (HOLA) to ultrasound scanning facilitates fast and detailed exploration of all venous circuits in pediatric patients3 (see Chapters 1 and 47). Preprocedural scanning starts with examination of the superficial and deep veins of both arms. When central venous access is needed, the forearm veins can be ignored and the evaluation may start directly at the antecubital area, where the cephalic vein is generally visible on the radial border. The brachial artery is located medially, and one or more brachial veins are usually identified adjacent to the artery. Approximately halfway between the elbow and axilla the veins can be more carefully evaluated for possible cannulation. The most easily accessible vein at this level is the basilic vein, which lies superficial and medial to the brachial veins. As the basilic vein approaches the axillary area, it progressively merges with the brachial veins to form the axillary vein. In the PICU, cannulation of the basilic vein is a preferable option because this vein is larger and located more distantly in relation to the artery and the median nerve than the brachial veins are. The cephalic vein is usually a poor choice for cannulation because it is superficial, small, and tortuous.5 However, all upper extremity veins should be evaluated sonographically in terms of (1) internal diameter, (2) depth (distance from the surface of the skin), (3) regularity of trajectory (a tortuous vein or a vessel with a sudden bend is a bad choice for cannulation), (4) proximity to other anatomic structures that may be accidentally punctured (e.g., brachial artery, median nerve), and (5) any preexistent abnormalities (e.g., thrombosis, anatomic variations). Two-dimensional, color Doppler, and compression ultrasonography techniques can all be applied to investigate the aforementioned parameters.2 When the patient is hypovolemic or the veins are smaller than expected, the sonographic examination should be repeated after placement of a tourniquet (quite tightened and placed at the axilla). The minimum size of venous catheter available for ultrasound-guided insertion is 3 Fr. When no arm vein reaches a diameter of 3 mm, cannulation should not be attempted in this area. Interestingly, neonates and small infants rarely have deep arm veins larger than 2 mm. Occasionally, some infants might have an axillary vein with a diameter of 3 mm or larger (at the level of the axilla). Preprocedural scanning continues by exploration of the infraclavicular area to visualize the axillary vessels in both the transverse and longitudinal planes (Figures 13-1 and 13-2). In this area the cephalic vein can be also evaluated at its union with the axillary vein. In children, both the axillary and cephalic veins can be cannulated quite easily at this level. In neonates and infants, these veins are usually too small for cannulation, although exceptions might occur, as mentioned in previous paragraphs. Scanning of the supraclavicular area starts at the middle of the neck by sweeping the transducer in a transverse plane over the internal jugular vein (IJV) and the common carotid artery (Figures 13-3 and 13-4). At this level the IJV is evaluated in terms of diameter, extent of collapse during breathing, position relative to the artery, presence of valves, and possible abnormalities (e.g., thrombosis, hypoplasia). By sweeping the transducer downstream (along the IJV trajectory) toward the lower neck region, the subclavian artery can be visualized as a major arterial segment that lies deeper than the IJV and in transverse alignment with the IJV trajectory. Next, the transducer reaches the suprasternal notch, where it can be tilted in a frontal orientation to scan the anterior mediastinum, at which point the brachiocephalic vein (almost longitudinal plane) is visualized (Figures 13-5 and 13-6). In neonates, the brachiocephalic vein is often the easiest and safest vein to cannulate because of its large diameter. By sweeping the transducer laterally (above the superior clavicular border) the subclavian vein (longitudinal plane) is visualized (Figures 13-7 and 13-8). In this area, especially in neonates and infants, the deep tract of the external jugular vein (longitudinal axis) becomes visible as a compressible structure that lies posterosuperior and parallel to the subclavian vein. Hence external jugular venipuncture may be easier and safer than subclavian venipuncture in view of the close proximity of the latter to the pleura. Once again, preprocedural scanning should evaluate all the aforementioned venous circuits (which are accessed in the neck area) in terms of diameter, distance from the surface of the skin, possible abnormalities, and other parameters as mentioned in previous paragraphs. Finally, the lower extremity is scanned accordingly only in the upper part of the thigh and the groin area. The most suitable veins for cannulation are usually the femoral and saphenous veins. Nevertheless, both veins can indeed be very small in underweight neonates and thus not suitable for cannulation. Ultrasound-based evaluation of all peripheral and central veins, which represent potential catheterization “targets,” is performed bilaterally. In expert hands a complete ultrasound examination may require just 2 minutes. Next, the same strictly aseptic, real-time ultrasound-guided method used in adults is also applied in children to obtain central venous access; however, various technical differences do exist. Figures 13-3 and 13-4 Visualization of the internal jugular vein and the carotid artery at the midneck region.
Pediatric ultrasound-guided vascular access
General considerations and ultrasound evaluation of peripheral and central veins in pediatric patients (preprocedural scanning)

Instrumentation and kits used for ultrasound-guided catheterization in neonates and children
Transducer
Related posts:
 Ultrasound-guided peripheral intravenous access
Ultrasound-guided peripheral intravenous access
 Ultrasound-guided arterial catheterization
Ultrasound-guided arterial catheterization
 Ultrasound-guided placement of inferior vena cava filters: (CONSULTANT-LEVEL EXAMINATION)
Ultrasound-guided placement of inferior vena cava filters: (CONSULTANT-LEVEL EXAMINATION)
 Use of ultrasound in the evaluation and treatment of intraabdominal hypertension and abdominal compartment syndrome
Use of ultrasound in the evaluation and treatment of intraabdominal hypertension and abdominal compartment syndrome
 Ultrasound imaging in space flight
Ultrasound imaging in space flight
 Procedural ultrasound for surgeons: (CONSULTANT-LEVEL EXAMINATION)
Procedural ultrasound for surgeons: (CONSULTANT-LEVEL EXAMINATION)
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Pediatric ultrasound-guided vascular access