Figure 17.1
Appendicitis. A blind-ended tubular structure with an outer diameter of greater than 5.7 mm

Figure 17.2
Diameter greater than 5.7 mm. The diameter in pediatric appendicitis is greater than 5.7 mm as measured in this figure

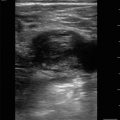
Figure 17.3
Target sign. When the appendix is inflamed, it can resemble a target with hypoechoic and hyperechoic concentric rings

Figure 17.4
Appendicolith. Hyperechoic foci within the lumen of the appendix that causes posterior shadowing

Figure 17.5
Appendicitis with periappendiceal fluid. Inflammatory fluid surrounds the appendix depicted by the arrow
Intussusception
- (a)
Indications
Colicky abdominal pain
Vomiting
Currant jelly stool
Lethargy
- (b)
Image Acquisition
Transducer selection:
Curvilinear
Phased array
Linear array: can be used with thinner patients
Patient position:
The patient should be supine with the head of the bed flat and their knees flexed to allow abdominal muscles to relax.
Place the transducer in the right lower quadrant, and follow the path of the large intestine:
It is rare to have an intussusception of the small intestine, though it is possible.
Alternatively, another way to evaluate for intussusception is to slide the transducer using an up-and-down lawn mower technique to cover the entire abdomen.
The majority of intussusceptions are located in the right upper quadrant.
- (c)
Pathology
Telescoping of one section of the bowel into another:
Commonly occurs at the ileocecal junction
Figure 17.6—Intussusception

Figure 17.6
Intussusception. In a longitudinal plane, there is an invagination of the bowel into itself causing a telescoping-like effect. This is commonly referred to as a “pseudokidney” as it looks like a kidney in appearance

Figure 17.7
Doughnut sign. In a transverse plane, there will be concentric alternating hypoechoic and hyperechoic rings representing layers of the bowel with adjacent free fluid and inner fecal matter
Pyloric Stenosis
- (a)
Indications
Projectile non-bilious vomiting:
Commonly occurs within the first weeks of life (4–8 weeks)
Palpable olive-shaped mass in the upper abdomen
- (b)
Image Acquisition
Transducer:
Linear array
Patient position:
The patient should be supine with the head of the bed flat.
Place the transducer in an oblique position over the epigastrium with the marker pointed toward the patient’s left shoulder:
Figure 17.8—Transducer placement for pyloric stenosis
Fan the transducer up and toward the right shoulder, and then fan the transducer down toward the right hip:
If the patient has a lot of bowel gas, use graded compression by exerting gentle pressure over the area of interest with the ultrasound transducer in effort to displace the bowel gas.
Or reposition the patient by placing them in the right lateral decubitus position to move air up into the fundus of the stomach and fluid down.
- (c)
Pathology
Get Clinical Tree app for offline access
Pyloric stenosis occurs when the pylorus becomes hypertrophied blocking food from exiting the stomach into the small intestine.
Identify the pyloric channel:
The outer thick muscular wall will appear hypoechoic compared to the more hyperechoic inner mucosa:
Figure 17.9—Pyloric stenosis short axisRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree