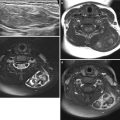
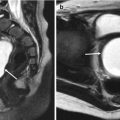
Fig. 27.1
Hydrometrocolpos in a 12-year-old girl with amenorrhea. (a) Longitudinal US shows a dilated, echogenic fluid-filled vagina and uterus. (b) T2-weighted sagittal MR image shows markedly dilated vagina and endometrial cavity with hemorrhage of intermediate signal intensity. (c, d) Contrast-enhanced coronal and sagittal CT scans show cystic dilatation of the vagina and uterus due to vaginal obstruction
27.4.2 Vaginorectal Fistula
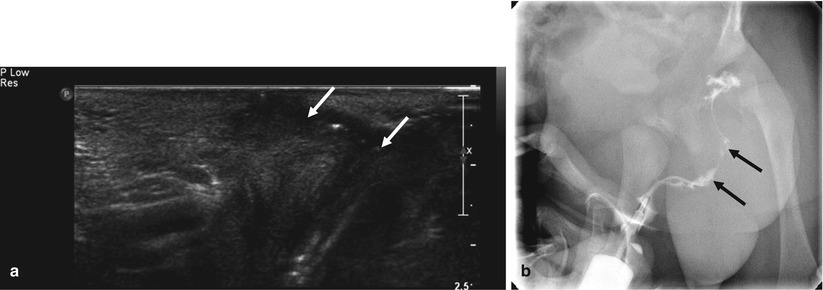
Fig. 27.2
Vaginorectal fistula in an infant with swelling and pus from labia. (a) Perineal US shows hypoechoic fistula tract with some hyperechoic air, connecting with rectum. (b) Fistulography shows contrast-filled, fistula tract from labia to rectum
27.4.3 Precocious Puberty
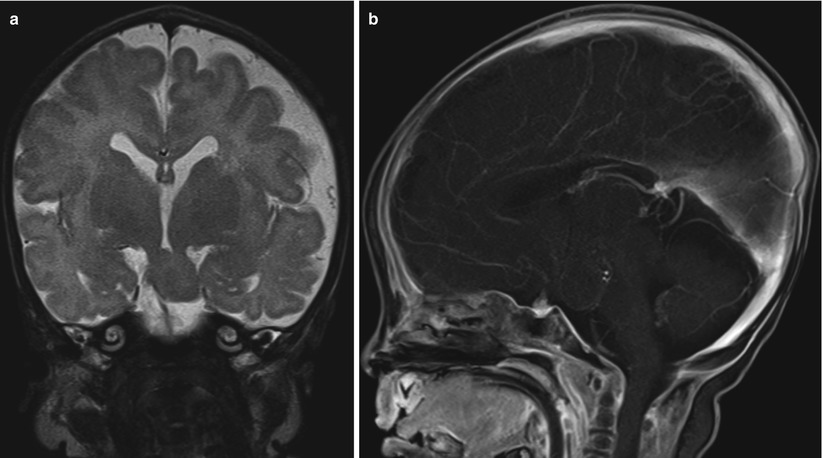
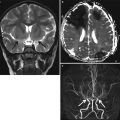
Fig. 27.3
Central precocious puberty in 5-year-old girl with vaginal bleeding. (a) T2-weighted coronal MR image shows focal mass at tuber cinereum. (b) Contrast-enhanced sagittal T1-weighted MR image shows no contrast enhancement of mass in tuber cinereum
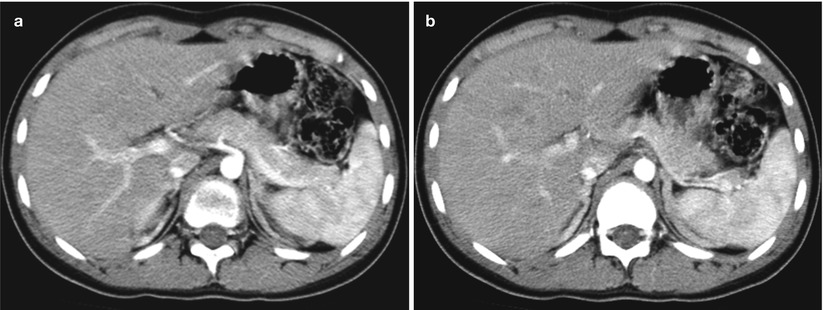
Fig. 27.4
Peripheral precocious puberty in 15-year-old girl with massive vaginal bleeding. (a) and (b) Contrast-enhanced axial CT scans show diffuse enlarged both adrenal glands, suggesting adrenal hyperplasia
27.4.4 Congenital Anomalies of Uterus and Vagina
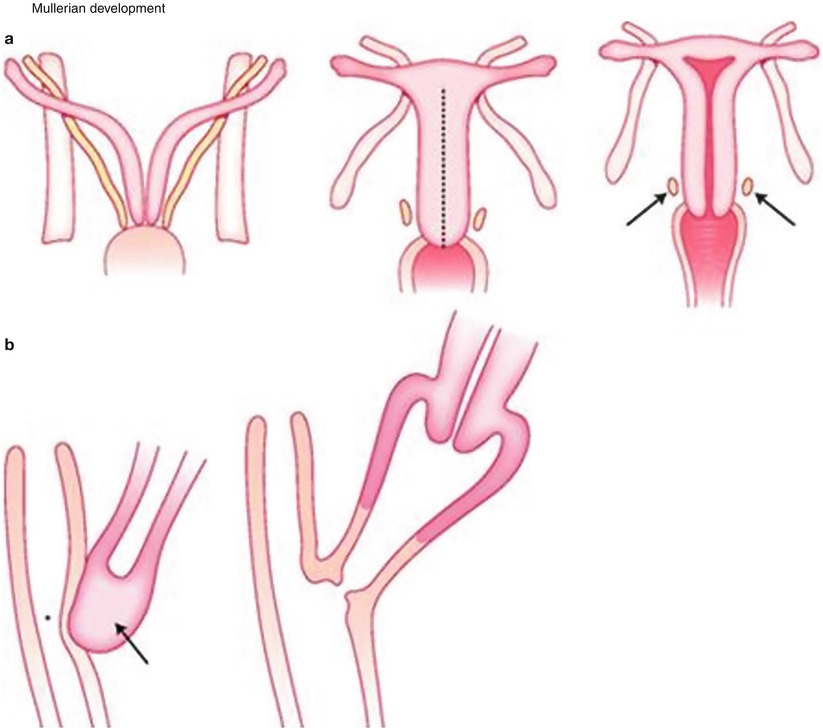
Fig. 27.5
Schematic drawing of müllerian development. (a) Both müllerian ducts (arrows) fuse on the midline to form the uterus. The proximal part of the duct gives rise to the fallopian tube. The Wolffian ducts (arrows) regress and the distal remnant of the Wolffian duct forms the Gartner duct. (b) This diagrams shows that the uterovaginal canal (arrow) reaches the urogenital sinus (asterisk). The vagina is formed by both the müllerian ducts and the urogenital sinus (From Radiology illustrated Gynecologic imaging)
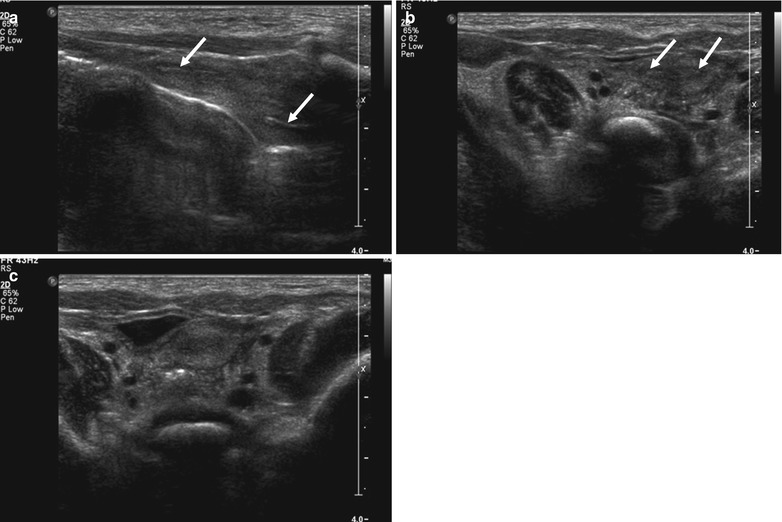
Fig. 27.6
US of a bicornuate uterus in a 2-month-old girl. (a) Oblique sagittal US shows two endometrial cavities in two horns. (b, c) Sequential axial US shows divergence of the uterine horns and a single uterine cervix
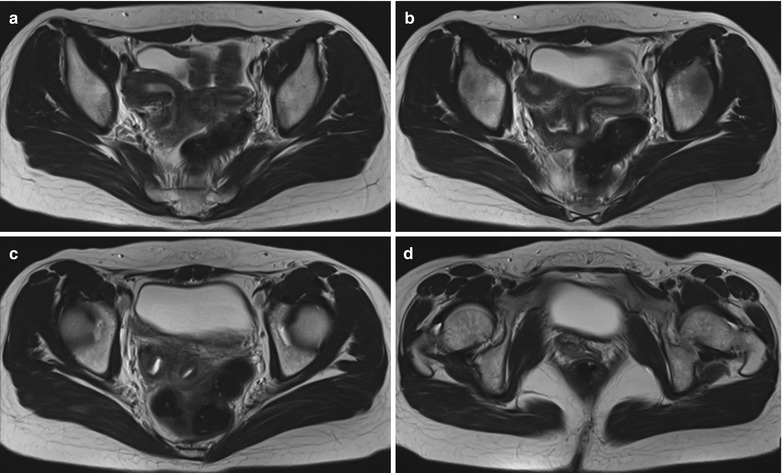
Fig. 27.7
Uterine didelphys in a 15-year-old girl. T2-weighted axial MR images of pelvis show two uterine horns (a, b), two cervices (c), two separate vaginal lumen (d)
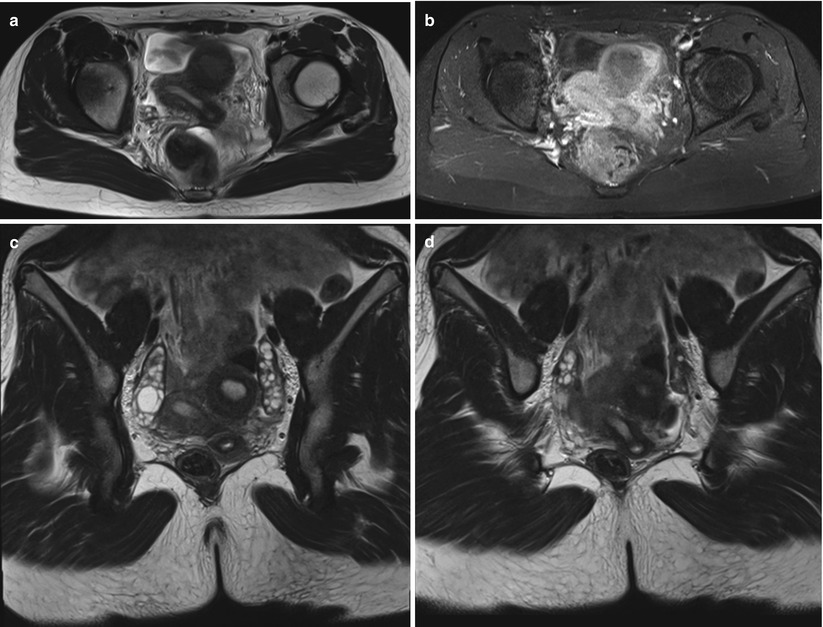
Fig. 27.8
Unicornuate uterus with noncommunicating rudimentary horn in a 14-year-old girl. (a, c, d) T2-weighted MR images show unicornuate uterus and separated rudimentary horn containing endometrial cavity not communicating to opposite horn. (b) Contrast-enhanced T1WI shows enhancing endometrium in unicornuate uterus and rudimentary horn

Fig. 27.9
Aplasia of the entire segments of uterus and vagina (Mayer-Rokitansky-Küster-Hauser syndrome) in a 14-year-old patient. (a) Midsagittal T2-weighted MR image reveals no vagina and uterus. (b) Axial T2WI at the level of the femur head shows no vagina between the bladder and the rectum
27.4.5 Tuboovarian Abscess
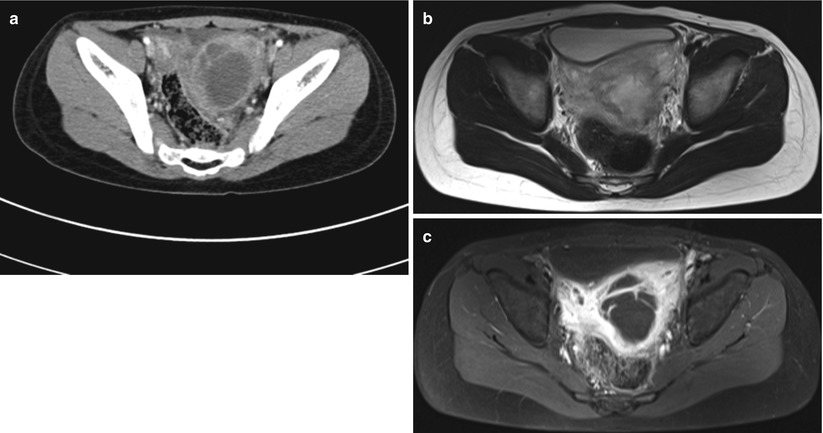
Fig. 27.10
Left tubo-ovarian abscess in an 11-year-old girl. (a) Contrast-enhanced CT scan shows a large cystic mass in left adnexa. This mass has thick wall and septa, and has poor demarcation from the adjacent organs, suggesting adhesion with the uterus and rectosigmoid colon. (b) Axial T2WI shows a thick-walled, septate, cystic lesion in the left adnexa containing heterogenous high signal intensity. (c) Contrast-enhanced T1WI reveals strong enhancement of the wall and septa of the lesion with infiltration of adjacent organs
27.4.6 Ovarian Torsion
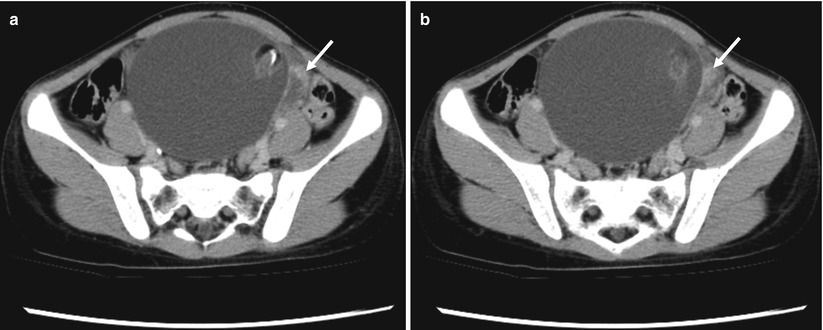
Fig. 27.11
Torsion of cystic mature teratoma in a 9-year-old girl. (a, b) Contrast-enhanced CT scans show cystic mass with fat and calcification and conglomerated vascular structure connecting the mass to the left uterine conus, which represents vascular congestion of the twisted pedicle (arrow). At surgery, there was 360-degree torsion and oophorectomy was performed
27.4.7 Hernia of Uterus and Ovary
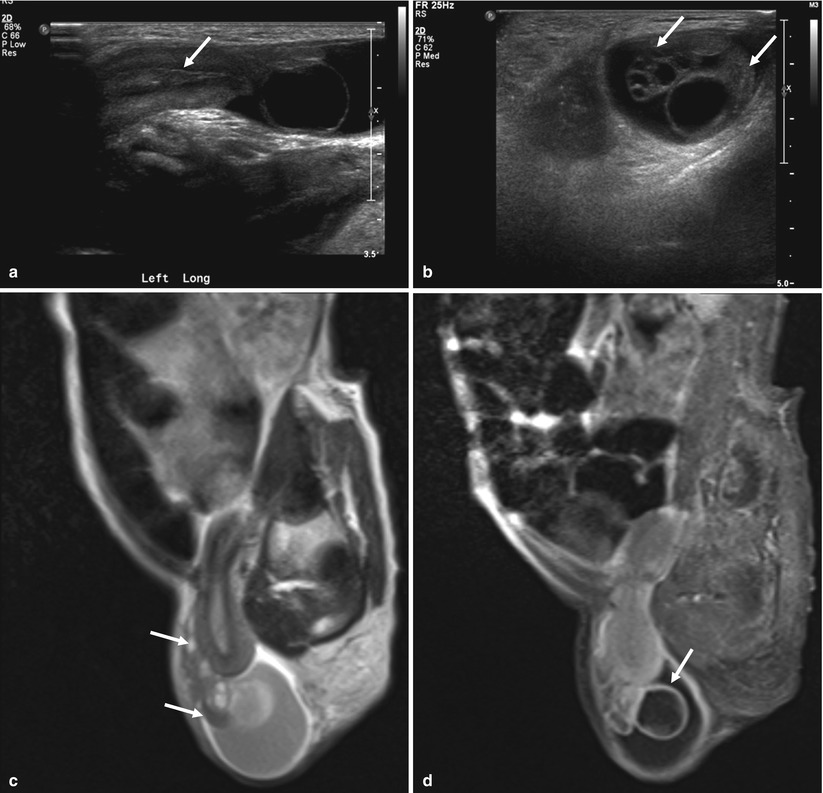
Fig. 27.12
Herniation of ovary and uterus in a 3-month-old girl. Longitudinal (a) and transverse (b) US images of left inguinal canal show a herniated uterus and two ovaries (arrows) with small cyst and multiple follicles. Sagittal T2WI (c) and contrast-enhanced T1WI (d) demonstrate a herniation of uterus and two ovaries (arrows in c) with multiple follicles and small follicular cyst (arrow in d)
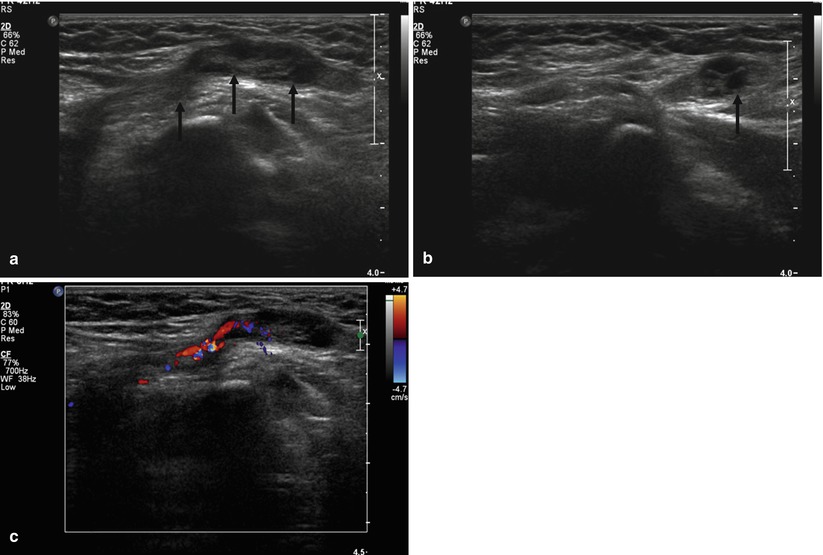
Fig. 27.13
Ovary herniation into the inguinal canal in a 1-year-old girl. Longitudinal (a) and transverse (b) US images of the left inguinal canal show a herniation of ovary with peripheral small follicles. Color Doppler (c) US demonstrates flow signals in the pedicle of the ovary.
27.4.8 Ovarian Cyst
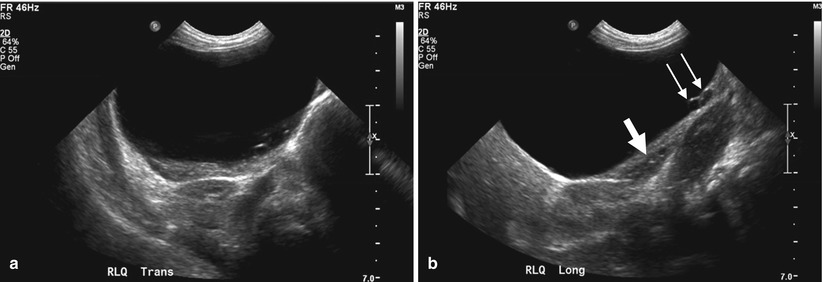
Fig. 27.14
Large ovarian cyst in a 3-month-old girl. (a) Transverse US of right lower abdomen shows a large cystic mass with imperceptible wall inferior to the kidney. The maximal diameter was about 7 cm. (b) Longitudinal US shows multiple daughter cysts (arrows) and ovarian tissue (thick arrow) in the peripheral portion of a large cyst of the left ovary
27.4.9 Ovarian Tumor: Germ Cell Tumor
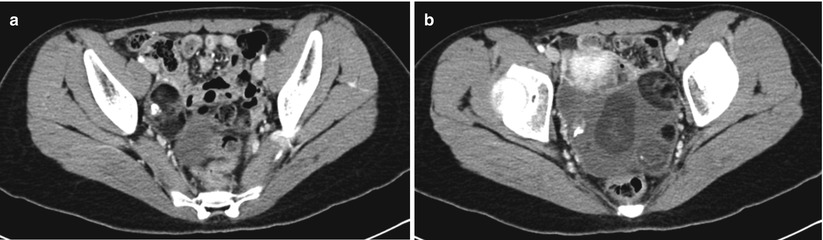
Fig. 27.15
Bilateral ovarian teratomas in a 15-year-old girl. (a) Axial contrast-enhanced CT scan shows a right ovarian mass containing fat and mural nodule with calcification. (b) Axial contrast-enhanced CT scan shows a left ovarian cystic mass containing fat, calcification, serous fluid, and mural nodule
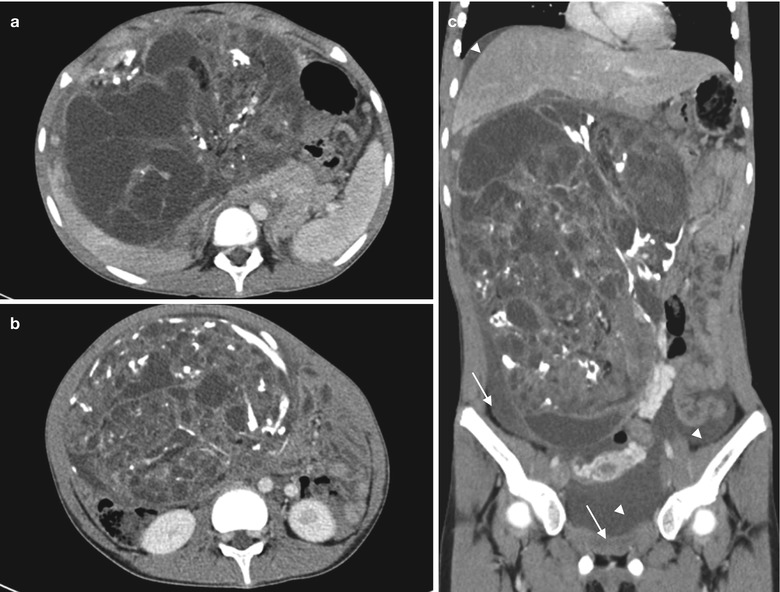
Fig. 27.16
Ruptured immature teratoma in a 13-year-old girl. (a, b) Contrast-enhanced CT scans show a huge, predominantly solid mass containing fat and calcifications filling the abdomen and pelvic cavity. (c) Coronal CT scan shows ascites (arrowheads), and peritoneal thickening with enhancement (arrows) suggest tumor seeding. Laparotomy revealed ruptured immature teratoma with peritoneal seeding
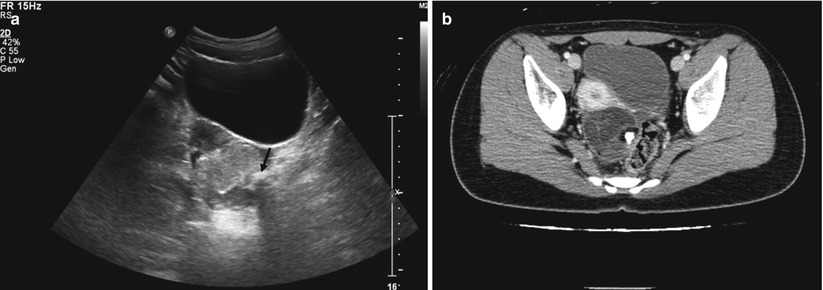
Fig. 27.17
Ovarian teratoma in a 13-year-old girl. (a) Transverse US of the pelvic cavity shows a echogenic mass containing hyperechoic nodule with posterior shadowing (arrow) suggesting calcification. (b) Contrast-enhanced CT demonstrates fat and calcification in the cystic mass. At pathologic examination, ovarian teratoma containing fat, hair, sebaceous tissue, and calcification was confirmed
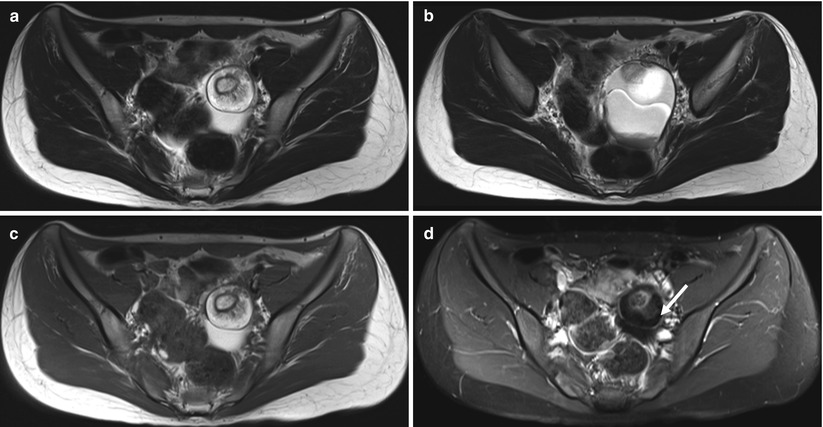
Fig. 27.18
Mature cystic teratoma in a 16-year-old girl. Axial T2-weighted (a, b) and T1-weighted (c) MR images show left ovarian cystic mass containing fat, calcification, and mural nodule. Contrast-enhanced, fat-suppressed, T1-weighted (d) image demonstrates strong suppression of the signal of fat (arrow)
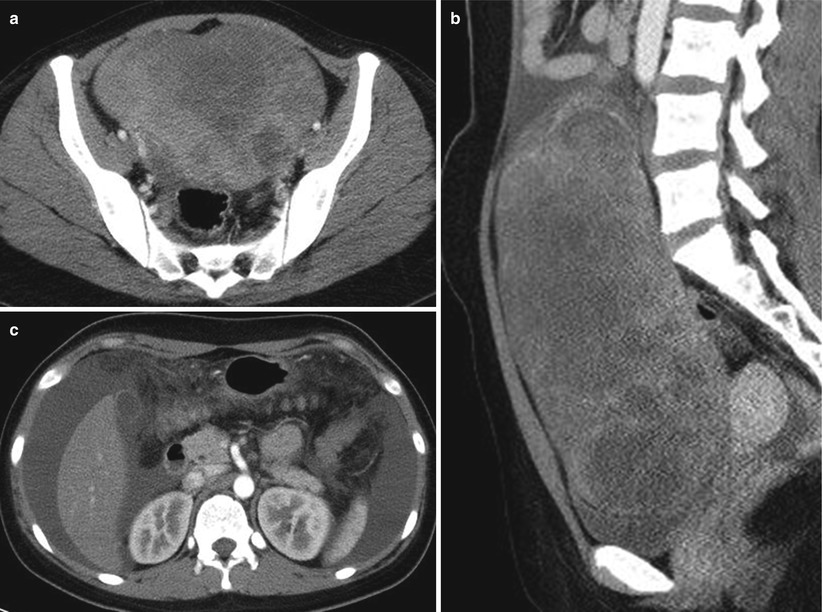
Fig. 27.19
Dysgerminoma of left ovary in a 15-year-old girl. (a, b) Contrast-enhanced axial and sagittal CT scans show a large solid enhancing mass in pelvic cavity. The mass has multifocal low-attenuation areas. (c) Contrast-enhanced axial CT scan of upper abdomen demonstrates large amount of ascites and ill-defined increased attenuation of omentum, suggesting peritoneal seeding
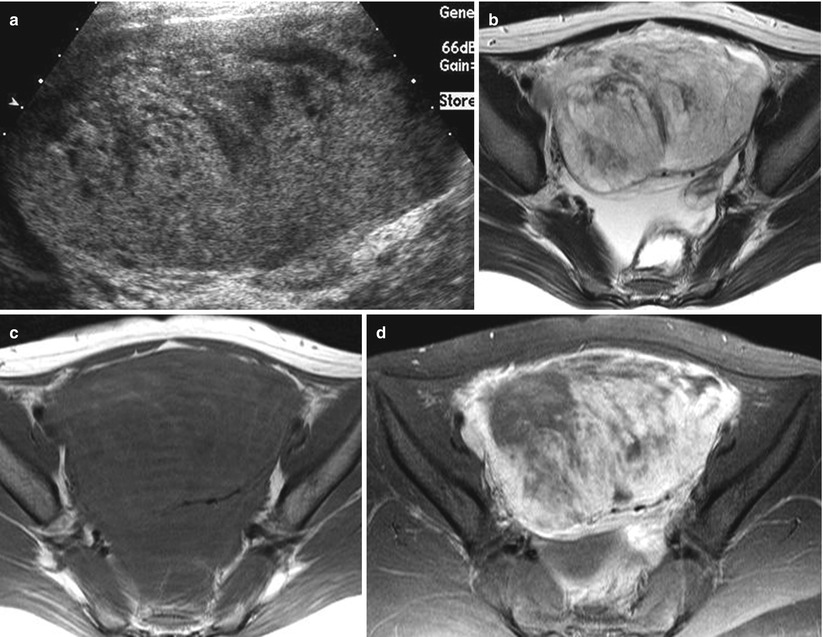
Fig. 27.20
Endodermal sinus tumor of right ovary in a 13-year-old girl. (a) Axial US scan of pelvis demonstrates solid mass with hypoechoic necrotic area. (b) T2-weighted axial MR image shows a large mass with heterogeneous signal intensity and small ascites in the pelvic cavity. (c) On T1-weighted axial MR image, this mass shows areas of high signal intensity due to hemorrhage. (d) On contrast-enhanced, fat-suppressed, T1-weighted axial MR image, this mass shows heterogeneous enhancement and irregular necrotic areas
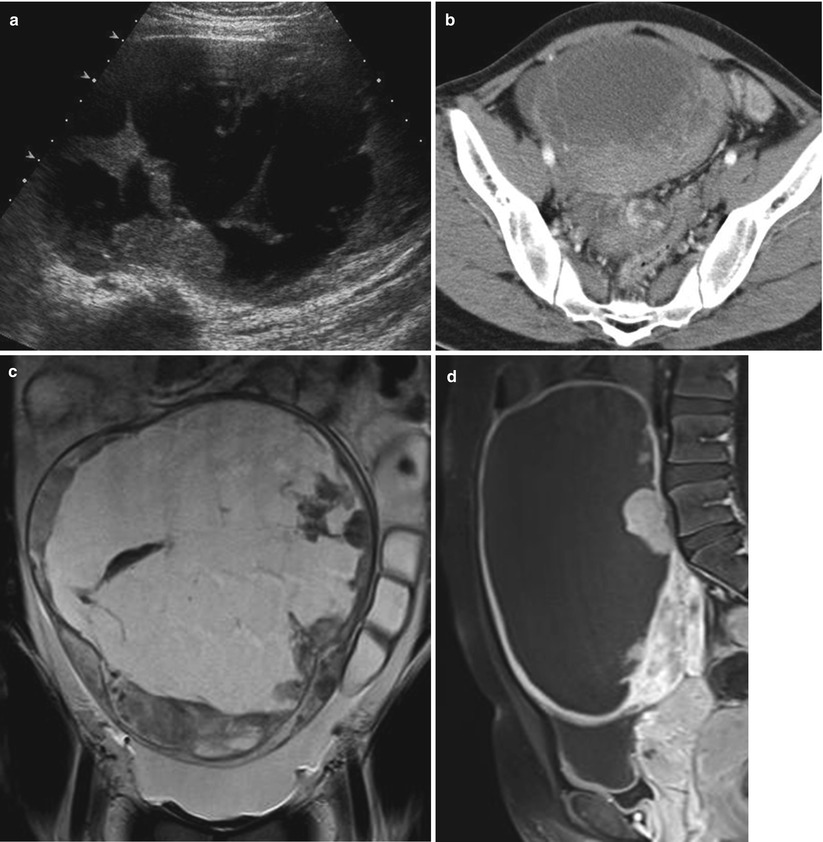
Fig. 27.21
Mixed germ cell tumor composed of dysgerminoma and endodermal sinus tumor in a 16-year-old girl. (a) Axial US scan of pelvis shows large cystic mass with septa and some solid portions. (b) Contrast-enhanced axial CT scan shows a large mass with enhancing septa and solid portions. (c) T2-weighted coronal MR image shows a huge, lobulated mass in the lower abdomen and pelvic cavity. This mass is mainly cystic and has some solid portions. (d) Contrast-enhanced, fat-suppressed, T1-weighted, sagittal MR image demonstrates huge cystic mass with enhancing thick wall and solid portions. The serum AFP was increased (3,000 ng/mm3)
27.4.10 Ovarian Tumor: Sex Cord-Stromal Tumor
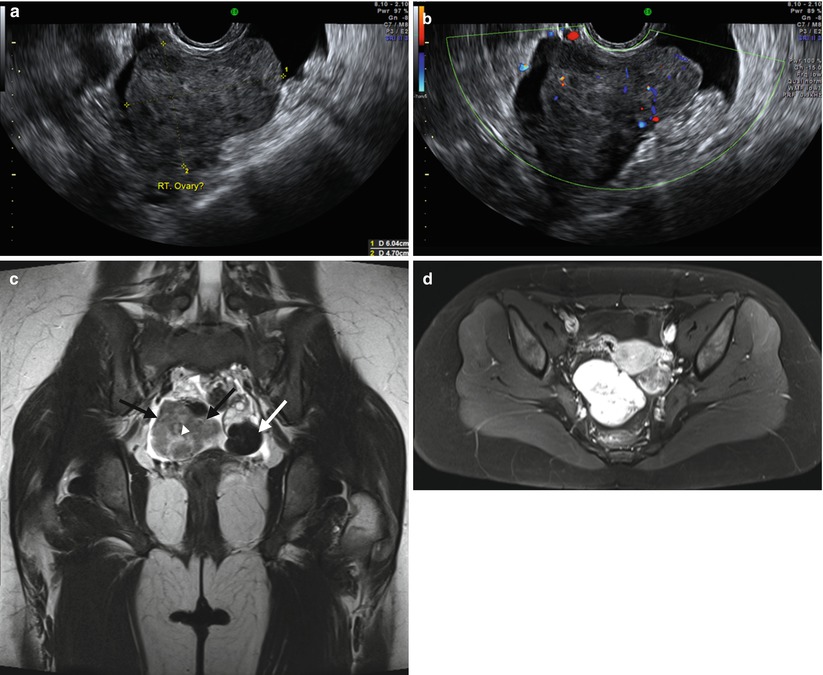
Fig. 27.22
Bilateral ovarian fibromas appearing as a predominantly solid mass in a 14-year-old girl. (a, b) Endorectal US scans of pelvis show a solid mass without increased color flow in right adnexa. Coronal T2-weighted (c) MR image shows a heterogenous low-intense, solid mass (dark arrows) containing central, high-intensity, necrotic foci (arrowhead) in right ovary and round, hypointense, solid nodule (white arrow) in inferior portion of left ovary. The signal intensity of the mass is very low, which is a characteristic finding of a fibrous tumor. There is small ascites in pelvis. (d) Axial contrast-enhanced T1WI demonstrates strong enhancement of ovarian solid masses
27.4.11 Ovarian Tumor: Epithelial Tumor
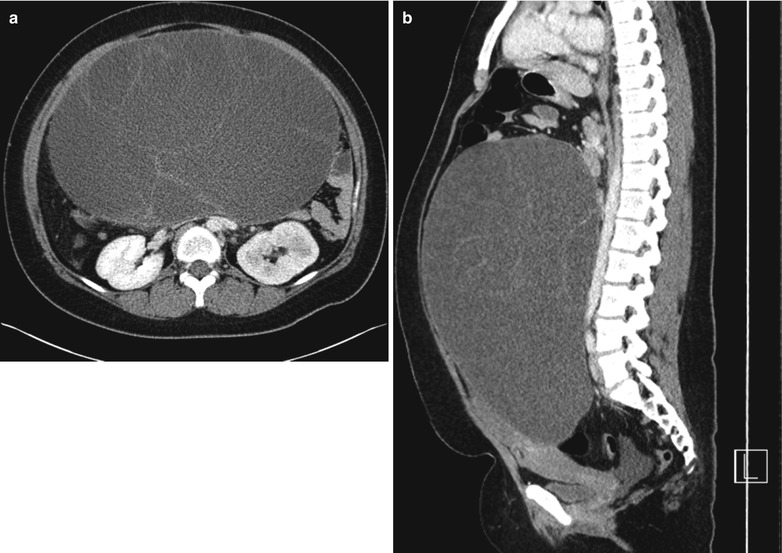
Fig. 27.23
Serous cystadenoma in a 16-year-old girl. Contrast-enhanced axial (a) and sagittal (b) CT scans show multiseptated, huge cystic mass displacing the uterus anteriorly. Note that the locules of the mass have similar attenuation
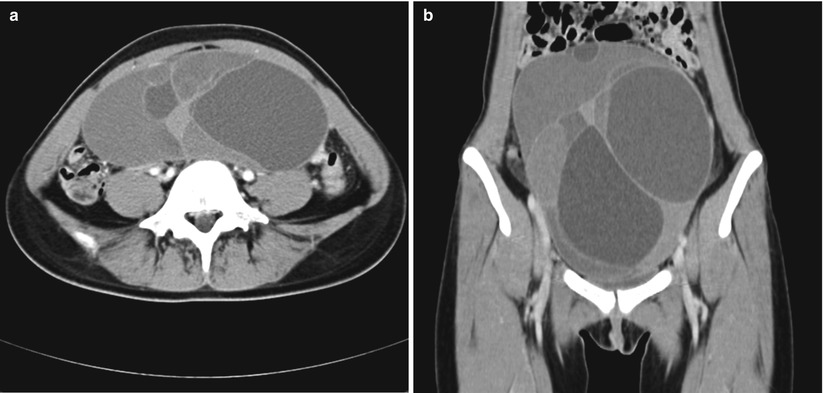
Fig. 27.24




Mucinous cystadenoma in a 18-year-old girl. Contrast-enhanced axial (a) and coronal (b) CT scans show multiseptated, huge cystic mass in abdomino-pelvic cavity. Note that the locules of the mass have different attenuations
Related posts:


Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
