Synovial cysts have long been known to create radicular pain in the spine, with the clinical effect mimicking a disk herniation. These cysts have traditionally been treated with open surgical therapy. Now a minimally invasive, image-guided approach to treatment is available to relieve this problem, using a simple percutaneous needle stick and injection. This article describes the technical aspects and precautions needed for this intervention.
Synovial cysts are extradural lesions that appear to arise from the synovial lining of the facet joints. The cause and mechanism of development are thought to be micromotion and microtrauma that are associated with degenerative changes within the facet joint. This condition leads to the rupture of synovial membrane and subsequent cyst formation caused by the leak of synovial fluid and cells. There is containment of this material with proliferation of mesenchymal cells and myxoid degeneration. The most common location of cysts is the L4-L5 level because it is the location reported to have the highest degree of spinal motion ( Fig. 1 ). These cysts are almost always associated with significant degenerative facet disease and, not uncommonly, a degree of degenerative spondylolisthesis is also present.

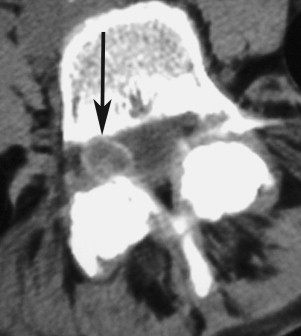
When they are small, synovial cysts are usually asymptomatic. However, there may be symptoms of back pain related to degenerative facet disease. As the cysts enlarge, they can compress the thecal sac or the exiting nerve root in the foramina. This compression may result in spinal stenosis and/or radiculopathy ( Fig. 2 ). Symptoms are usually unilateral but, with progressive spinal stenosis, bilateral symptoms can also occur. Bilateral cysts are rarely present (see Fig. 2 ). Synovial cysts are unusual in higher locations (cervical and thoracic) but can produce myelopathy when present.

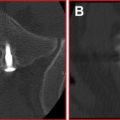
The differential diagnoses of cyst-like lesions in this location include arachnoid cysts, perineural (Tarlov) cysts, schwannomas, disk fragments, ganglion cysts, cysts of the ligamentum flavum or posterior longitudinal ligament, and pseudocysts. The most common cyst in the L4-L5 area is the synovial cyst. Arachnoid cysts are more common in the thoracic region. Tarlov cysts and schwannomas have direct association with the nerve root and are generally found away from the facet joint. Schwannomas enhance uniformly, whereas a synovial cyst will show rim enhancement only. Most cysts will be high signal on T2 and low signal on T1 magnetic resonance (MR) images (see Figs. 1 and 2 ). Atypical signal patterns occur because calcification in the rim (and sometimes center) of the cysts is not uncommon ( Fig. 3 ). In addition, air can occasionally be found inside these cysts and comes from the degenerative facet joint.
Synovial cysts are conspicuous on MR imaging, and this method is currently the most common method of diagnosis. Computed tomography (CT) can also be used for diagnosis but is less common now. Increased awareness of this lesion and its conspicuous nature on an MR image make it a progressively more common diagnosis.
Treatment options
Traditional therapy has been surgical microdecompression and removal of the symptomatic synovial cyst. Surgery by removal of the compression on the adjacent structure works well for pain relief. However, surgery alone does not address the facet degeneration or spondylolisthesis (if present). If spondylolisthesis is present, surgical fusion to address the slip may be indicated. In the Mayo Clinic experience (involving 194 patients), 91% of the patients had good pain relief, and 84% experienced improvement in motor deficits. However, complications included 4 patients subsequently requiring fusion because of spondylolisthesis that developed after laminectomy, cerebrospinal fluid leak (in 3 patients), discitis (1 patient), epidural hematoma (1 patient), seroma (1 patient), deep vein thrombosis (1 patient), and a death caused by cardiac arrhythmia.
Percutaneous facet or cyst injection (without cyst distension or rupture) has been reportedly successful in some patients, but the recurrence of symptoms is high. In a long-term follow-up, it was seen that the condition of approximately only one-third of the patients improved. Most patients had poor outcomes, and more than half of them went on to undergo surgery.
Percutaneous injection of the synovial cyst with attempts at rupture or overdistension has also been reported in various articles. In each of these articles, there is improved outcome compared with using an injection alone. Two studies respectively report 75% and 72% long-term good outcomes with injection. Some patients had recurrence of pain and went on to have a second attempt at cyst rupture. The least encouraging study reported that approximately 50% of patients in their series had long-term benefits. This number is an improvement when compared with using an injection alone, with these patients avoiding surgery. The patients treated with injection and cyst rupture and who improved had long-term outcomes similar to patients who had surgery. As reported in the Mayo Clinic experience, surgery was not without notable complication. This risk seems to be averted in the percutaneous group making a first attempt at cyst rupture a reasonable, less invasive choice.
Percutaneous technique
This procedure is performed with the patient in the prone position. The patient’s skin is prepared with a sterile solution. Because the procedure is often transiently painful (during cyst distension), conscious sedation is commonly used. This sedation is preceded by a preoperative workup and perioperative monitoring. Preoperative antibiotics may also be administered; usually, 1 g of Ancef is given intravenously.
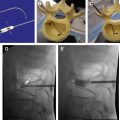
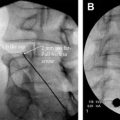
Image guidance for this procedure can be obtained with either fluoroscopy or CT. Fluoroscopy gives real-time visualization of needle placement but is problematic because the cyst can usually not be visualized directly. However, contrast injection into the facet joint (that the cyst communicates with) usually opacifies the cyst. One can then directly stick the needle into the cyst (via an interlaminar approach) or attempt distension and rupture by injecting into the facet joint directly. Direct puncture of the cyst seems to have a greater likelihood of creating enough pressure to rupture the cyst, but both techniques have been successful.
CT guidance, like fluoroscopy, has its advantages and disadvantages. Contrast resolution is better with CT, frequently allowing the cyst to be seen before direct injection ( Fig. 4 ). Needle placement into the facet joint is also facilitated because the 3-dimensional contour of the facet joint is better demonstrated with CT. The cyst can be accessed via injection into the facet joint itself ( Fig. 5 ). Direct puncture of the cyst via an interlaminar approach can also be accomplished with CT ( Figs. 6 and 7 ), but the gantry angle required to allow this approach may be problematic. This latter problem has been minimized with the use of CT fluoroscopy.