(1)
Department of Radiology, John H Stroger Jr Hospital of Cook County, Chicago, IL, USA
Peritonitis
Diagnosis
Bacterial Peritonitis
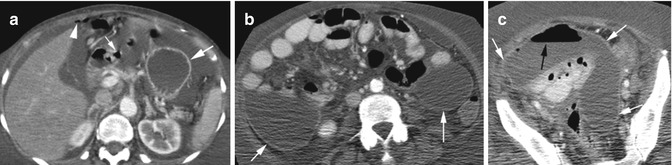
Fig. 16.1
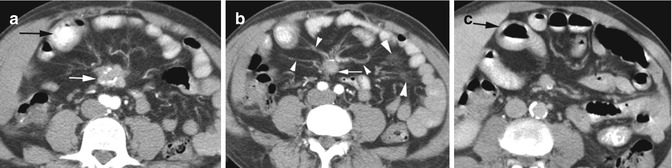
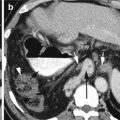
Bacterial peritonitis from ruptured duodenal ulcer. CT axial (a) shows small pneumoperitoneum (arrowhead) with perforation of the first part of duodenal sweep (thin white arrow). The stomach shows ischemic changes with only the mucosa enhancing (thick arrow). Fluid is seen in the peritoneal cavity with mild peritoneal enhancement. (b, c) Later date axial CT shows peritonitis of the mid-abdominal and pelvic peritoneum which now shows increased enhancement and thickening (white arrows) with increased intraperitoneal gas collection (black arrow)
Imaging Features
1.
Peritoneal fluid collection
2.
Enhancement of peritoneum
Diagnosis
Bile Peritonitis
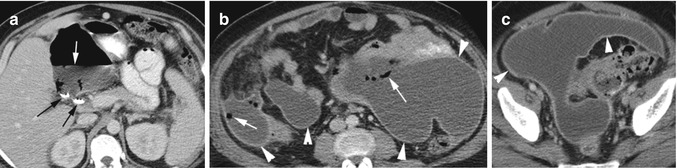
Fig. 16.2
Bile peritonitis with superimposed infection from recent cholecystectomy. Axial CT (a–c) images show large amount of ascites with thick enhancing peritoneum (arrowheads) and with gas collection (white arrows). The gas is predominant in the gastrohepatic space adjacent to the cholecystectomy clips (black arrows)
Pneumoperitoneum
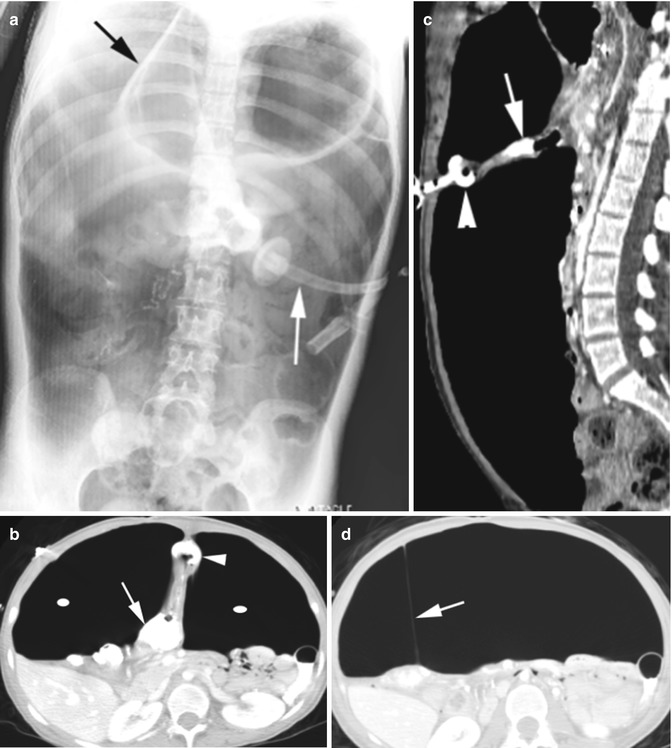
Fig. 16.3
Pneumoperitoneum from gastrocolocutaneous fistula and peritoneal leak from malposition of gastrostomy tube. (a) Flat plate of abdomen shows large pneumoperitoneum surrounding the falciform ligament (black arrow) and the gastrostomy tube (white arrow). CT axial (b) and sagittal (c) reformatted images show gastrostomy tube (arrowhead) connected to the colon (arrow). The large peritoneal gas (ellipse) is displacing and compressing the bowel loops. (d) Axial CT showing falciform ligament (arrow) with surrounding pneumoperitoneum
Hemoperitoneum
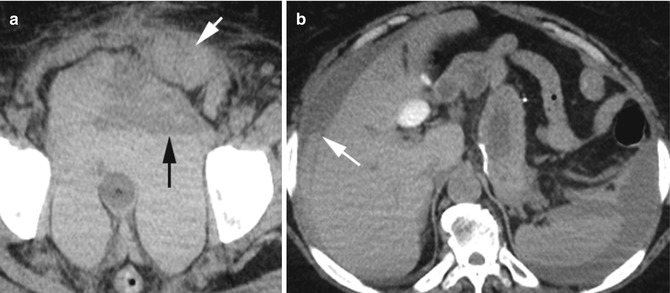
Fig. 16.4
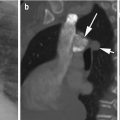
Hemoperitoneum. Patient on Coumadin for PE and high INR had trauma. CT axial (a) image shows large hemoperitoneum in posterior cul-de-sac with hematocrit level (black arrow). Large hematoma in left rectus abdominis muscle (white arrow). Axial CT of upper abdomen (b) shows hemoperitoneum with hematocrit level in right subphrenic space (white arrow)
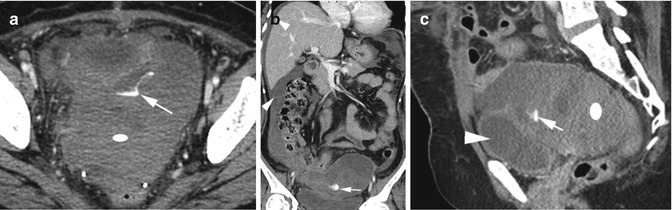
Fig. 16.5
Active arterial bleeding. CT axial (a), coronal (b), and sagittal (c) reformatted images show active extravasation of contrast (arrow) from a branch of the internal iliac artery surrounded by high-density lobulated sentinel clot (ellipse). The rest of the peritoneal cavity is filled with lower density hemorrhagic fluid (thin arrowheads) but of higher attenuation than urine in the bladder (thick arrowhead)
Chylous Ascites
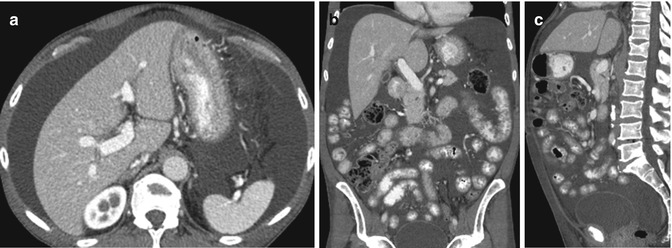
Fig. 16.6
Chylous ascites: CT axial (a), coronal (b), and sagittal (c) reformatted images show low-density ascites distending the peritoneal cavity with no lymphadenopathy. Milky fluid was tapped. Cause not known
TB Peritonitis

Fig. 16.7
TB peritonitis in different patients. Patient 1: CT axial (a, b) and coronal reformatted (c) images show thickening of the omentum (long white arrow) and small bowel mesentery (short white arrows) with vascular congestion. Peritoneal fluid is surrounded by enhancing peritoneum (arrowhead). Patient 2: Axial CT (d) shows nodular thickening of peritoneum (arrow). Patient 3: Axial CT (e) shows very thickened omentum with prominent vessels (white arrow) which are also seen on the peritoneal surface (black arrow). Patient 4: Axial CT (f) shows enlarged lymph nodes in the retroperitoneum (white arrows), thick peritoneum (arrowhead), and thick omentum (black arrow)
Peritoneal Lymphomatosis
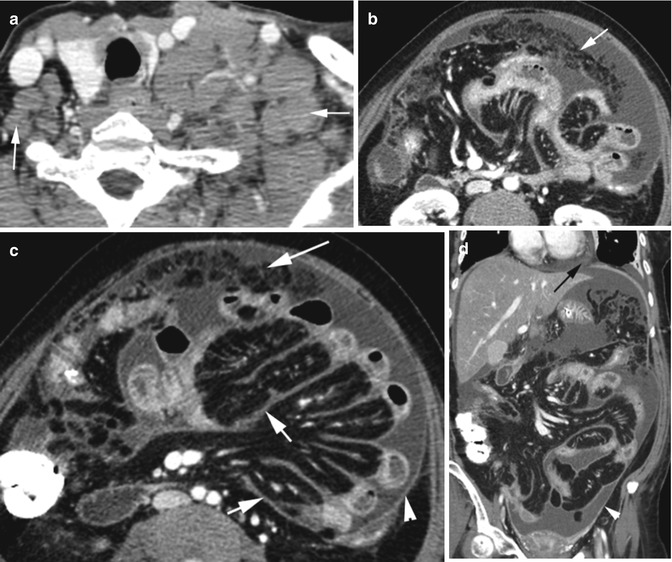
Fig. 16.8
Peritoneal lymphomatosis. Patient with diffuse large B-cell lymphoma. CT (a) axial image of the neck shows large lymph nodes in the supraclavicular region more on the left side (arrow). CECT of the abdomen, axial (b, c) and coronal reformatted (d) images show moderate ascites, omental increased markings (long white arrow), and diffuse thickening of leaves of the mesentery (short arrows) displacing small bowel loops. Peritoneum shows enhancement (arrowhead); small pericardial fluid (black arrow) is seen. No abdominal lymphadenopathy
Mucinous Ascites
Diagnosis
Perforated Mucocele Appendix
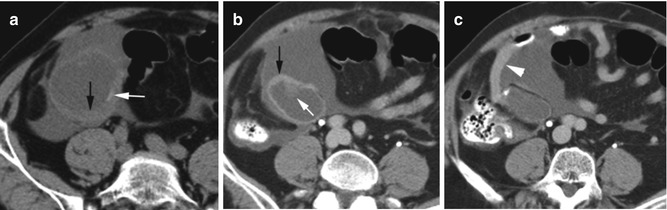
Fig. 16.9
Perforated mucocele appendix. Axial CT (a) noncontrast image shows dilated mucus-filled thick-walled (black arrow) appendix with a faint curvilinear calcification (white arrow) surrounded by extruded mucus. Delayed phase axial CECT (b, c) shows mild enhancement of the irregular thick wall (black arrow) and soft tissue mural nodule (white arrow). The extruded mucus is causing extrinsic pressure on the adjacent small bowel (arrowhead)
Diagnosis
Pseudomyxoma Peritonei
Imaging Features
1.
Diffuse low-density peritoneal mucinous ascites with soft tissue strands
2.
Scalloping surface of liver, spleen, and mesentery
3.
Rim-like or punctate calcifications
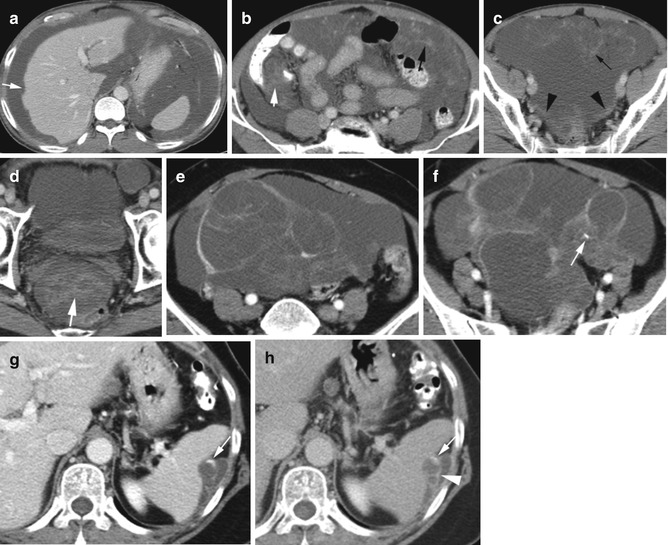
Fig. 16.10
Pseudomyxoma peritonei in two patients. Patient 1: Axial CT (a–d) shows the peritoneal cavity is distended with low-density fluid. Stranding (thin black arrows) in the fluid is mostly in the ileocecal region (short white arrows) and pelvis (thick white arrow) with thick peritoneum in the posterior cul-de-sac (arrowheads) and scalloping liver surface (thin white arrow). Patient 2 with perforated mucinous cystadenoma of the appendix: Axial CT (e, f) show thick septation in the mucinous ascites and a focal calcification (arrow). (g, h) Axial CT of the same patient with recurrence after 2 years shows septated mucinous tumor (arrowhead) with rim-like calcification (white arrow) in left subphrenic space scalloping on the spleen surface
CSF Pseudocyst
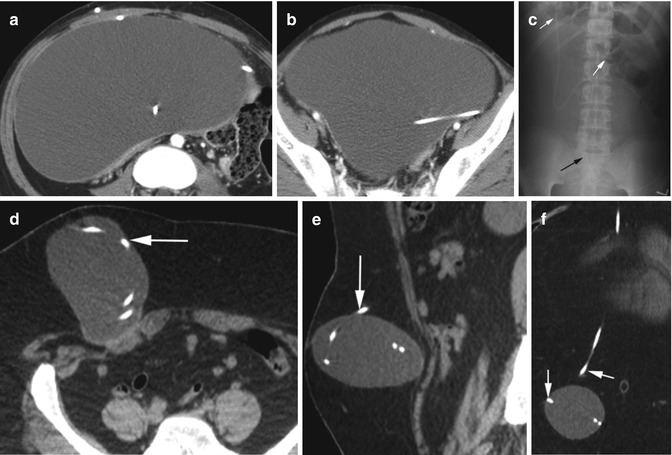
Fig. 16.11
CSF pseudocyst. Patient 1: Axial CT (a, b) show a large thin-walled cystic mass around the ventriculoperitoneal shunt catheter. (c) Flat plate of the abdomen shows large fluid collection around the VP shunt displacing bowel loops (white arrows), with the tip of the catheter at the level of the right SI joint (black arrow). Patient 2: CT (d) axial, (e) sagittal, and (f) coronal reformatted images show the shunt catheter is coiling in the subcutaneous tissue in the right lower abdominal wall (arrow) surrounded by well-marginated fluid collection
Mesenteric Lesions
Sclerosing Mesenteritis
Diagnosis
Retractile Mesenteritis