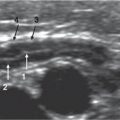
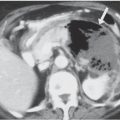
Fig. 2.130 Peritonitis secondary to free perforation of acute appendicitis. Sagittal US image of pelvis in a 3-year-old boy shows echogenic fluid surrounding the hyperechoic omentum and intestinal loops over the distended bladder. The appendix was not identified, even at surgery.Fig. 2.131 Douglas fluid. Sagittal US image shows a small amount of hyperechoic free fluid in the pouch of Douglas (arrowhead) in a patient with suspected acute appendicitis. This finding suggests this diagnosis, particularly if seen after 48 hours of evolution, even if the appendix itself is not depicted. In this case, surgery confirmed the diagnosis of acute appendicitis.Fig. 2.132a, b Tuberculous peritonitis. US abdominal scans at mesogastrium (a) and RLQ (b) show the thickened hyperechoic omentum located in contact with the whole anterior abdominal wall. In (a), the omentum is seen homogeneously hyperechoic, whereas in (b) it is more heterogeneous. Slightly echogenic ascites is present. Note that in appendicular peritonitis, the omentum is in contact with the appendicular area, not the abdominal wall.Fig. 2.133a, b Meconium peritonitis. Transverse abdominal US through the right upper quadrant (RUQ) (a) and in mesogastrium (b). Ascites is present. In (a), the meconium deposits are seen in subdiaphragmatic area. In (b), meconium is seen beside the left kidney. Also in (b), the bowel loops are outlined by a thin hyperechoic meconium rim.
Table 2.61 Localized fluid collections See Tables 2.64and 2.66(abdominal cystic masses) and free peritoneal air (pneumoperitoneum) in neonate.
Diagnosis
Findings
Comments
NEC
Air dissecting colonic wall with free air in late stages.
Seen in premature infants.
Gastric perforation
Large amount of peritoneal air.
Spontaneous idiopathic perforation in premature infants.
GI tract obstruction
Obstruction is evident.
Usually in low tract obstruction: imperforate anus, Hirschsprung disease, meconium ileus.
Extra-abdominal air dissection
From pneumomediastinum.
Iatrogenic
After laparotomy, thermometer injury in rectum, traumatic tube placement in stomach or bladder.
Table 2.62 Free peritoneal air (pneumoperitoneum) in neonates
Diagnosis
Findings
Comments
GI tract perforation
Location of air depends on location of perforation.
After gastric or duodenal ulcer, appendicitis, inflamed Meckel diverticulum.
Extra-abdominal air dissection
From pneumomediastinum.
Iatrogenic
After surgery.
Fistulas
To abdominal wall, GI tract, vagina.
Air-producing intra-abdominal infections
Gas may be contained or disseminate to peritoneum.
In emphysematous infections: appendicitis, pancreatitis, other origin abscesses, etc.
Table 2.63 Peritoneal calcifications
Diagnosis
Findings
Comments
Tumors
Neuroblastoma
Over 30% of tumors show coarse or stippled calcifications. Most common locations: paravertebral and suprarenal.
Up to 70% of tumors have calcifications on CT exam.
Teratoma
Coarse calcifications, but also frequently well-defined structures, like teeth.
Also fat density can be depicted in radiograph.
Wilms tumor
Mass effect in the renal fossa, with curvilinear or phlebolithic calcifications in 15%.
Calcifications are not stippled.
Hepatoblastoma
Heterogeneous, coarse, ill-defined calcifications in 12%–30%. In some cases, osseous matrix.
Also, hemangioendothelioma may show fine granular calcifications. Hepatoma has no calcium on radiograph.
Mesenteric cysts
Rim calcification.
Inflammatory—trauma
Calcified abscesses
Frequent in paravertebral tuberculous abscesses, less frequent in bacterial.
Secondary to spondylodiscitis.
Tuberculous peritonitis
Small foci of calcifications in multiple locations.
Usually other signs of TB (in most cases pulmonary) are not seen.
Calcified hematoma
Usually posttrauma.
Hydatid cysts
Eggshell-like calcification, most of them located in the liver, but also splenic, peritoneal.
Caused by calcification of external (adventitial) layer. In endemic areas.
Meconium peritonitis
Small flecks of calcification scattered throughout abdomen. Lineal calcifications along inferior surface of liver.
In neonates, with obstructive signs following birth. Pathologic obstetric US. Also accompanied with meconium pseudocysts.
Peritoneal dialysis
Lineal calcifications of peritoneum.
Deposit of calcium-binding protein after several years of dialysis.
Lymph nodes
Single or multiple, usually in central or lower abdomen, rounded or irregular.
After a wide variety of infections: TB, salmonella, other bacteria.
Other
Phlebolith
Small, rounded calcifications with central radiolucent dot.
Frequent in pelvis.
Renoureteral calculi
Irregular or rounded calcifications of variable sizes, located superimposed to the kidneys and to the ureteral trajectory.
Uric acid stones only show calcification with CT.
Biliary calculi
Rounded calcification, usually multiple and sometimes with central low-density area.