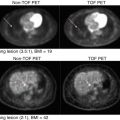
Fig. 17.1
A young male patient with a mediastinal germ cell tumour. 18F-FDG-PET/CT (a) and PET/MRI (b) transaxial images through the upper thorax
17.3 Underlying Tumour Biology and FDG
The progression from a few cancer cells to the formation of macroscopic solid tumours is a complex process of activation of specific metabolic pathways providing oxygen, glucose, other nutrients and growth factors which are critical for the growth of cancer cells [28]. Sokoloff et al. were the first to report FDG in their work on measuring regional cerebral glucose metabolism in animals using 14C-deoxyglucose autoradiography [29]. Subsequently FDG was developed for PET imaging which provided similar quantification of regional concentrations in humans. It was the Warburg observations in the 1930s, showing a high rate of glycolysis in cancer cells, which led to use of FDG as a tumour imaging agent. There is a complex process which regulates the multiple factors that influence the rate of glucose flux which can be measured by FDG-PET [30].
Membrane transporters for glucose are involved in the uptake of FDG by the cell. FDG is then phosphorylated by hexokinase to form FDG-6-phosphate in the cell. Unlike glucose-6-phosphate, FDG-6-phosphate is metabolically trapped and does not undergo further significant enzymatic reactions [31]. The primary exception to metabolic trapping of FDG is in the liver, where a large concentration of phosphatase enzymes results in dephosphorylation of FDG-6-phosphate and clearance of FDG from hepatocytes [32, 33]. Being a polar molecule, it cannot easily pass through the cell membrane to be redistributed out of the cell. With high levels of glucose-6-phosphatase, the phosphate group is cleaved off to regenerate FDG which can diffuse out of the cell and is redistributed elsewhere. Studies have shown FDG uptake for most tumours is mediated by (Fig. 17.2):

Fig. 17.2
Principles of 18F-FDG metabolism and signal amplification: like glucose, 18F-FDG is transported into the cells by the glucose transporter (GLUT-1); however, this happens at a much higher rate. This is then phosphorylated by hexokinase II (HK-II) to form 18F-FDG-6-PO4. Unlike glucose, further metabolism is arrested due to the presence of fluorine at the carbon-2 position of the ring instead of the hydroxyl group in glucose. 18F-FDG-6-PO4 does not enter the standard metabolism that glucose-6-PO4 does, and hence it remains trapped within the cell. This “metabolic trapping” of 18F-FDG-6-PO4 within the cell leads to signal amplification and forms the basis of the analysis of PET data
- (a)
Increased levels of membrane transporters for glucose (especially GLUT-1)
- (b)
Increased levels of hexokinases (HK-II)
- (c)
Stable or low levels of glucose-6-phosphatase (G-6-Pase) [34]
It has been shown that aberrant glycolysis decreases metabolic stress-induced apoptosis and leads to uncontrolled proliferation of cancer cells which is essential to the malignant tissue phenotype [35]. There is debate on the relative importance of glucose transporters versus the hexokinase activity in predicting the FDG uptake rate in cancer cells [36]. However, both in vitro and in vivo studies have shown that it is the phosphorylation status, and not the membrane transporters, that determine the rate of FDG uptake in most circumstances [37, 38].
As the tumour grows, hypoxia occurs and this is usually present 100–150 μm from the nearest blood supply. Hypoxia and rapid tumoural cell growth force the cells to be dependent on the anaerobic metabolism of glucose. This adaptive behaviour of tumour cells is one of the most crucial steps in tumour survival and progression [39]. There are various proposed molecular targets which are involved in tumourigenesis, and one such factor is hypoxia-inducible factor (HIF)-1, also known as pro-survival transcription factor. HIF-1 has two subunits, HIF-1α and HIF-1β, of which HIF-1α undergoes rapid degradation under normoxic conditions and the β subunit is the one which is constitutively expressed [40]. However, under hypoxic conditions, HIF-1α is stable and undergoes dimerisation with HIF-1β to form an active transcription factor. This dimer binds to the promoter of target genes, i.e. DNA sequence 5′-RCGTG-3′ (hypoxia response element, HRE), which leads to activation of angiogenic pathways, tumoural progression pathways and overexpression of glycolytic enzymes and vascular endothelial growth factor (VEGF) [39, 41]. Tumour hypoxia is one of the most important factors leading to an increased rate of FDG metabolism by anaerobic glycolysis [40]. The understanding of active molecular pathways involved in accelerated cellular proliferation such as mitogen-activated protein kinases and reduced apoptosis like AKT (alpha serine-/threonine-specific protein kinase) in carcinogenesis are shown to be responsible for rapid glucose uptake for glycolysis [42]. These pathways are well known to stimulate glycolysis. Studies have shown that as the AKT activity decreases, there is associated decline in the transcription of glycolytic enzymes, including GLUT transporter expression [43, 44].
There are other features which have led to widespread use of FDG in the clinical setting [8]. Unlike glucose, FDG is filtered and excreted by the kidneys leading to substantial clearance of FDG within 1 h of administration. Increased levels of the highly active hexokinase enzyme effectively trap FDG from the blood pool and are responsible for FDG retention in tumours in a short period after injection. This combined effect of increased tissue uptake and rapid blood pool clearance of FDG forms the basis of the resultant high-contrast images [45]. Most clinical oncology PET imaging protocols allow 60–90 min after the injection of FDG for tissue uptake and background and blood pool clearance before image acquisition [46].
Regional glucose metabolism can be quantified in detail using the dynamic PET imaging method which measures FDG accumulation in the tissue of interest for 60–90 min after injection to produce a tissue uptake curve [46]. This can be combined with direct arterial activity sampling or image-derived arterial activity (e.g. left ventricle or aorta) so that physiological rate constants can be estimated by applying compartmental modelling to these data sets [47, 48]. The metabolic rate of FDG can then be quantified in mmol/min/g [29, 33]. Dynamic imaging of FDG is time consuming and difficult for patients in clinical practice, and it is not possible to extend acquisitions over the whole body with current scanners field of view [46]. Whilst dynamic imaging and arterial sampling is valuable for research applications, the most commonly used clinical imaging method is a single image acquisition of FDG uptake after 60–90 min after injection over a number of consecutive bed positions to cover the required extent of the body [46]. This static uptake image gives an approximate indicator of glucose metabolism [29, 33]. The uptake can be measured semi-quantitatively as the standardised uptake value (SUV) which can be calculated as SUV = Ct/(i.d./wt), where Ct is the tissue FDG uptake from the image (kBq/mL or μCi/ml), i.d. is injected dose (e.g. MBq) and wt is the patient weight (kg). A uniform distribution of tracer is represented by an SUV of 1, and SUV > 1 is an indicator of specific accumulation of tracer [46, 48]. Tumours show variable uptake but most untreated lesions have SUVs of 3 or higher [49]. However, there is overlap between benign and malignant tumours and other non-malignant pathological processes including inflammation [49, 50]. The 110 min half-life of 18F allows regional distribution of FDG from a central cyclotron and radiochemistry facility. Keeping in mind all these attributes, FDG is the most commonly used clinical oncological imaging agent [51].
Currently the Centers for Medicare and Medicaid Services (CMS) recommends the clinical applications of FDG-PET in initial and subsequent treatment strategies of most common cancers such as colorectal, oesophagus, thyroid, head and neck, lymphoma and non-small-cell lung cancers. A few other cancers such as cervix, melanoma and breast are covered with exceptions and are reimbursable under CMS [10, 11].
17.4 Beyond FDG
Over decades FDG has played an indispensable role in clinical oncology. However, other PET tracers contribute to the molecular imaging abnormal tumour biology as there are known limitations of FDG [8]. Apart from imaging FDG-based energy metabolic changes related to tumour growth, there are various other biological pathways such as tissue repair, hypoxia, angiogenesis, apoptosis, cell invasion and migration which are not directly reflected with FDG-PET imaging [52]. The future of oncological therapy includes targeted therapies and individualised management which may need more specific PET radiopharmaceuticals that will help us guide personalised patient treatment by prediction and quantification of therapeutic response and identification of factors causing therapeutic resistance [53, 54]. Many more isotopes/molecules/markers and techniques are being constantly studied and are set to revolutionise personalised medicine. These have most potential in oncology, immunology and neurological disorders [19, 55].
17.4.1 PET Tracers for Imaging Tumour Amino-Acid Metabolism
Similar to increased glucose uptake and metabolism, tumour cells also have upregulation of protein synthesis and increased expression of the cell membrane transporters involved in transport of the amino acids [56]. Upregulated amino-acid metabolism forms the basis of amino-acid-based targeted PET imaging. The radiolabelled amino-acid tracers are metabolised and transported across the cellular membranes in a similar way to endogenous amino acids [57]. The major route providing amino-acid transport is the sodium-independent amino-acid transport system L, and studies have shown that tumour cells exhibit upregulation of L-type amino-acid transporter 1 (LAT1) expression. Increased LAT1 as a target has been used for PET tumour imaging [58]. PET imaging using amino acids includes natural and synthetic amino acids.
17.4.2 Natural Amino Acids
Of the various natural amino acids which are radiolabelled, the role of L-[methyl-11C] methionine (11C-Met) has been extensively evaluated in oncology [59]. 11C-Met was first developed by Comar et al. in 1976 [60]. Kubota et al. reported the first study which showed the potential role of 11C-Met in the diagnosis of lung cancer [61]. Following this, Sasaki et al. demonstrated the potential role of 11C-Met in differentiating various grades of astrocytomas. A recently published study from Koizumi et al. found that 11C-Met has a predictive role in recurrent rectal cancer treated with carbon ion radiotherapy (CIRT) [62]. 11C-Met-PET imaging has shown promising results in detection and delineation of viable tumour, especially in low-grade gliomas. Recent studies have shown that 11C-Met-PET imaging has a promising role in the clinical management of cerebral gliomas, not only for initial diagnosis, grading, prognostication and therapy planning but also for differentiation of tumour recurrence, biopsy planning, surgical resection, radiotherapy planning and assessment of response to therapy [63–65] (Fig. 17.3). Other clinical indications which are under evaluation include the differentiation of benign and malignant lesions in head and neck cancer, melanoma, ovarian cancer and other tumours [66, 67]. However, the short physical half-life of 11C-Met prevents its use in most nuclear medicine departments unless there is an on-site cyclotron [7].

Fig. 17.3
A patient with a low-grade left frontal glioma. There is low 18F-FDG uptake (left) compared to normal brain cortex but a much greater tumour-to-background ratio with the 11C-methionine scan (right)
17.4.3 Synthetic Amino Acids
Due to inherent limitations of labelled natural amino acids, synthetic labelled amino-acid analogues have been developed. These synthetic amino-acid tracers can be classified into two groups: aromatic amino acids and non-aromatic amino acids. These are non-metabolisable compounds which show limited or no efflux from the cellular compartment leading to high accumulation and better imaging properties [68, 69].
Radiolabelled aromatic amino-acid tracers are usually tyrosine or phenylalanine primarily system L substrates. These include L-3-18F-alpha-methyl tyrosine (18F-FMT), 2-18F-fluoro-L-tyrosine (18F-TYR), O-(2-18F-Fluoroethyl)-l-tyrosine (18F-FET) and 6-18F-fluoro-L-3,4-dihydroxyphenylalanine (18F-FDOPA) [70]. 18F-FET and 18F-FDOPA have been extensively evaluated in humans. 18F-FET and 18F-FDOPA-PET/CT have demonstrated promise for assessing brain tumours, particularly low-grade gliomas where FDG shows limitations. 18F-FET-PET is found to be 92 % specific and 92 % sensitive for differentiating grade I and II recurrent gliomas from grade III and IV recurrent lesions [71]. 18F-FET-PET is also found to be a valuable prognostication marker in operated cases of glioblastoma multiforme [72].
Similarly, 18F-FDOPA-PET has shown utility in clinical brain tumour imaging and is found to have a sensitivity of 96 %, as opposed to 61 % for FDG for detection of primary and recurrent brain tumours [73, 74]. 18F-FDOPA has potential to differentiate low-grade from high-grade tumours and has been used to evaluate extracranial neuroendocrine tumours [75, 76].
Another category of synthetic amino-acid tracers includes alicyclic amino acids and 1-amino-cycloalkane-1-carboxylic acids; they are neither metabolised nor readily incorporated into protein [77]. There are various alicyclic amino-acid tracers that have demonstrated value in human imaging including 1-amino-cyclobutane-1-carboxylic acid (ACBC) and its 3-fluoro analogue anti-1-amino-3-18F-fluorocyclobutane-1-carboxylic acid (anti-18F-FACBC) and 1-amino-cyclopentane-1-carboxylic acid (ACPC). Anti-18F-FACBC, a leucine analogue, has been studied in human glioblastoma multiforme lesions with promising results [77]. Due to its minimal renal excretion compared to FDG, it has also shown promise in genitourinary cancer imaging, including prostate cancer, renal cell carcinoma and pelvic malignancies [78, 79]. Increased uptake of anti-18F-FACBC in renal papillary cell carcinoma is shown to differentiate it from clear cell carcinoma [80]. There is growing evidence to support the potential utility of 18F-FACBC as it has shown superior ability to target prostate cancer when compared to ProstaScint and 11C-choline PET/CT [79, 81]. In detecting recurrent disease in prostate cancer, 18F-FACBC has shown improved sensitivity compared to 11C-choline PET/CT [79]. Anti-3-18F-FACBC is found to be 89 % sensitive (36 patients) for detecting tumours in the prostate bed and 100 % sensitive in detecting an extraprostatic recurrence (10 patients) [82]. Studies in animals have shown that 18F-FACBC-PET imaging is not only useful in detecting prostatic cancers but also in differentiation of tumoural lesions from inflammatory pathologies and benign prostatic hyperplasia [83].
17.5 PET Tracers for Imaging Phospholipid Metabolism
Choline is a precursor of phosphatidylcholine and uptake correlates with cell proliferation [84]. Choline is an essential component of cell membrane phospholipid synthesis. Tumours, including prostate cancer, have an increased requirement for cell membrane synthesis, and it has been shown that prostate cancer cells have an increased intracellular transport of choline, increased choline kinase expression and increased choline metabolism [85, 86]. This led to introduction of carbon-11 choline (11C-choline) as a promising PET tracer for evaluation of various malignancies such as brain tumours, lung cancer, gastrointestinal and genitourinary malignancies and particularly prostate cancer. 11C-choline overcomes some of the limitations of FDG which is excreted through the urinary system which leads to increased background activity in the pelvis [87]. At the same time, it matches FDG in differentiating benign from malignant pathologies. All these features make 11C-choline an important tracer for imaging prostate cancer [88, 89] (Fig. 17.4). Other applications include meningiomas, head and neck and primary hepatic malignancies [88, 90]. Another choline tracer is 18F-choline which has a longer half-life in comparison to that of C-11 and is extensively used to study patients with biochemical recurrence of prostate cancer and has potential to be used as a marker of therapeutic response in prostate cancer with bone metastases [91, 92].

Fig. 17.4
11C-choline MIP image. A man with metastatic prostate cancer showing abnormal 11C-choline activity in a large primary prostate tumour with lymph node metastases in the pelvis and multiple bone metastases
17.6 PET Tracers for Imaging Tumour Angiogenesis
Angiogenesis which is pivotal for tumourigenesis is defined as the formation of new blood vessels from existing vascular structures [93]. The increased cellular proliferation in tumours needs an increased supply of metabolites and at the same time removal of metabolic waste products. Tumour hypoxia is the key factor which triggers neoangiogenesis and is found to be caused by proangiogenic growth factors [94]. The resultant neovasculature is disordered and usually does not meet the needs of the growing tumour leading to deoxyhaemoglobin and lactacidosis [93, 94].
Tumour angiogenesis is a complex multistep process which involves multiple growth factors which are involved in the activation of endothelial cells, degradation of basement membrane, migration of endothelial cells and angiogenic remodelling and vessel formation [95]. Some of the most important factors which are involved in neoangiogenesis are vascular endothelial growth factor (VEGF), epidermal growth factor receptor (EGFR), the acidic and basic fibroblast growth factors (aFGF and bFGF) and platelet-derived endothelial cell growth factor (PD-ECGF); these growth factors are secreted by tumour cells or by the fibroblast and endothelial cells in the peritumoural environment and extracellular matrix (ECM) [96]. Overexpression of the dimeric transmembrane integrin αvβ3 by activated endothelial cells occurs with angiogenesis. This integrin regulates endothelial cell migration and the matrix metalloproteinase (MMPs) family in matrix degradation, facilitating cell invasion, and angiogenesis. These molecules form the basis for targeted imaging of angiogenesis and the development of tracers for tumour angiogenesis imaging [97].
Dynamic 15O-water PET has been used to study tumour blood flow in vivo, as a pharmacodynamic marker to study the mechanism of novel anticancer drugs such as endostatin and to monitor delivery of radiolabelled drugs to the target [98, 99]. 15O-water is the gold standard for assessment of blood flow/tissue perfusion and provides a physiological measure. 15O-water PET not only provides information regarding the pharmacokinetics but also assess whether single agent of combination therapies have different effects on tumour perfusion [100, 101]. Other molecules used for imaging tumour vascularity include 11C-carbon monoxide but has logistic issues and low signal-to-noise. 11C-carbon monoxide PET is reported to measure blood volume up to approximately 0.1–0.2 ml blood ml−1 tissue in renal cancer which is characterised by a high vascular phenotype [102]. Anderson and co-workers reported the rapid changes in blood volume following treatment with combretastatin A4 phosphate (CA4P) [103].
Integrins are a family of heterodimeric cell surface receptors (24 subtypes) composed of two non-covalently bound α- and β-subunits involved in cell-extracellular matrix and cell-cell interactions [104]. Integrins mediate these by transducing signals into the cells and out of the cells directly or indirectly regulating cellular functions such as cell survival, proliferation, adhesion, migration and invasion as well as angiogenesis, thrombosis, apoptosis and differentiation in various pathological processes [104, 105]. Many cancer cells have been found to overexpress the integrin αvβ3, which binds to arginine-glycine-aspartic acid (RGD)-containing components of the interstitial matrix such as vitronectin, fibronectin and thrombospondin [104]. Upregulation of these pathways has been shown in melanoma, ovarian cancer and late-stage glioblastomas. Based on these findings, linear as well as cyclic RGD peptides, which show very high binding affinity and selectivity for integrin αvβ3, have been labelled with positron-emitting radionuclides to serve as PET radiotracers [105, 106]. Initial studies revealed tumour-specific uptake but also significant hepatobiliary elimination leading to high background activity in the hepatic parenchyma and small bowel. To improve the pharmacokinetics of these radiohalogenated peptides, several modifications have been attempted, including labelling with sugar moieties, hydrophilic amino acids and polyethylene glycol (PEG) [107]. One such example is a glycopeptide based on cyclo (Arg-Gly-Asp-D-Phe-Lys). In an integrin-positive M21 melanoma xenograft model, 18F-galacto-RGD showed integrin αvβ3-specific tumour uptake. Initial safety studies of 18F-galacto-RGD in humans have been performed, and it is found to specifically delineate integrin-positive lesions, and its good tumour-to-background ratio suggests that it can be used as a surrogate marker of angiogenesis [108]. In various tumour studies, no obvious correlation was found between FDG and 18F-galacto-RGD, and it was shown that integrin αvβ3 expression and glucose metabolism were not closely correlated in tumour lesions. Hence, imaging based on these traces provides complementary information in cancer patients [109, 110]. Newer tracers such as 18F- and 64Cu-labelled RGD-containing peptides have shown better pharmacokinetics, tumour uptake and retention of the RGD peptides [111, 112]. For example, compared to a non-PEGylated ligand 64Cu-DOTA-RGD, PEGylated RGD peptide 64Cu-DOTA-PEG-3400-RGD is found to have low hepatic and small bowel uptake with no significant change in tumour-specific uptake and retention and hence was suitable for visualising lesions above the liver [113]. PEGylation using 18F-FB-PEG3400-RGD PEGylation showed significant and prolonged tracer retention in tumour without any comprise on the desired rapid clearance [113].
A series of multimetric RGD peptides labelled with 18F have been developed for PET imaging and have improved pharmacokinetics, tumour uptake and retention patterns. One such example is the dimeric RGD peptide-based tracer 18F-FB-E[c(RGDyK)]2 (18F-FRGD2) [114]. In small-animal imaging, it showed predominant renal excretion, and when compared with the monomeric tracer 18F-FB-c(RGDyK), it showed nearly twice as much tumour uptake. A comparison of monomeric and dimeric RGD analogues with tetrameric RGD peptide-based tracer, 18F-FB-E[E[c(RGDfK)]2]2 in xenograft-bearing mice revealed significantly higher receptor binding affinity and faster clearance from blood pool, better metabolic stability, predominant renal excretion and significant receptor-mediated tumour uptake providing better tumour contrast [115, 116].
Recent advances in radiolabelled nanoparticles, including inorganic and organic nanoparticles targeting integrin αvβ3, are a newer class of probes shown to have a potential role in research as well as clinical oncology [117]. Examples of these tracers include inorganic single-walled carbon nanotubes (SWNTs) coated non-covalently with PEG and with cyclic RGD peptides and DOTA for 64Cu chelation which have unique size, shape and physical properties [118, 119]. These properties of SWNTs make them a promising material that can be used for multimodality imaging, such as PET/CT, PET/MRI and PET/optical imaging [120].
Another important angiogenic process studied and used for imaging is the VEGF/VEGF receptor signalling pathway. The development of VEGF- or VEGFR-targeted PET imaging probes could serve as an important tool for understanding VEGF/VEGFR in angiogenesis-related tumourigenesis and drug delivery and assessing response to therapy with anti-angiogenic agents [121, 122]. Tracers such as 124I-labelled VG76e, which is an IgG1 monoclonal antibody against human VEGF, have been used in PET imaging of solid tumour xenograft models. However, this had the limitation of poor immune reactivity [123]. Another tracer, 124I-labelled HuMV833, has shown success in the phase I trials [124]. Recent development of bevacizumab labelled with 111In and 89Zr for SPECT and PET imaging, respectively, has led to better understanding of angiogenesis in human ovarian cancer xenograft models [125]. VEGF121 labelled with 64Cu has been used for VEGF receptor expression, and 1,4,7,10-tetraazacyclododecane-N,N′,N″,N″′-tetraacetic acid (DOTA)-VEGF121 has been used for receptor-specific imaging for VEGFR-2 [126]. Small-animal PET imaging using 64Cu-DOTA-VEGF121 has been validated in small U87MG tumours showing increased expression of VEGFR-2 [127]. Tracers such as15O-water and 13N-NH3 are used for dynamic PET blood flow imaging and have been applied in brain tumours to study anti-angiogenic therapy and grading of tumours [128–130].
17.7 PET Tracers for Imaging Tumour Hypoxia
The presence of hypoxic/anoxic regions is a characteristic feature of 50–60 % of locally advanced solid tumours and has been described in a wide range of human malignancies, including cancer of the breast, uterine cervix, vulva, head and neck, prostate, rectum and pancreas as well as in brain tumours, soft tissue sarcomas and malignant melanomas [131, 132]. Tumour hypoxia is orchestrated by the transcription factor hypoxia-inducible factor (HIF)-1, which has been verified as a master regulator of oxygen homeostasis under hypoxic conditions. The resulting adaptive changes in the proteome and genome of the tumour cells are believed to lead to more aggressive clones which are better adapted to survive in the compromised environment. Subsequent selection and clonal expansion of these cells lead to a more adapted and aggressive tumour cell population [133].
Hypoxia has also been shown to reduce chemotherapeutic and radiotherapeutic efficacy by causing cells within hypoxic regions to cycle more slowly and by providing a selection mechanism for cells with reduced susceptibility for apoptosis [134]. As therapeutically modifying hypoxia may have potential to change therapy outcome in patients, non-invasive PET imaging for identification and quantitation of tumour hypoxia status could play a key role in predicting and monitoring treatment response [135, 136].
Of the non-invasive imaging modalities to image hypoxia, radionuclide studies using PET tracers are the most extensively studied [137]. Parametric PET hypoxia imaging of tissue using inhalation of 15O2 by measuring regional oxygen extraction fraction and metabolic rate is shown to be more accurate than the invasive methods [137, 138]. 15O2 PET imaging is currently a “gold standard” for non-invasive imaging of tissue oxygen levels; however, because of logistics and technical issues such as very short half-life of 15O2 (∼2 min) and also being an expensive technique, it is not widely used in experimental or clinical settings [139]. Nitroimidazoles have shown very high selectivity in targeting hypoxic tissue and also have radiosensitising properties [140]. Nitroimidazole derivatives such as pimonidazole or 2-(2-nitro-1H-imidazol-1-yl)-N-(2,2,3,3,3-pentafluoropropyl) acetamide (EF5) can be analysed using invasive methods such as immunohistochemical analysis or cell-sorting techniques [141]. The first reported PET tracer used for hypoxia imaging focused on radiolabelled 2-nitroimidazole analogues. Intracellular reductases reduce these tracer analogues into reactive intermediary metabolites, accumulation of which shows an inverse correlation with the level of tissue oxygenation. The formed intermediary molecules form covalent bonds with thiol groups of the intracellular proteins and tend to accumulate in hypoxic cells. Many nitroimidazole compounds with varied properties have been developed and tested in imaging hypoxia [142, 143].
18F-labelled fluoromisonidazole (18F-FMISO) was the first hypoxia PET tracer which was found to have tumour specificity. It has been extensively used both in preclinical and clinical studies [144]. Preclinical studies in the 36B10 glioma rat xenograft model have evaluated the role of 18F-FMISO uptake in hypoxic tumours and assessment of hypoxic fraction. It was found that retention of the 18F-FMISO correlated with the degree of tissue hypoxia [145]. Another study performed in a rhabdomyosarcoma rat xenograft model correlated 18F-FMISO uptake with other markers of hypoxia such as pimonidazole and carbonic anhydrase IX (CA IX). 18F-FMISO-PET was found to be accurate in measuring hypoxia and correlated well with the hypoxic volumes derived from pimonidazole- and CA IX-stained tumour sections [146]. Clinical studies evaluating the role of 18F-FMISO and FDG in head and neck cancer patients found no correlation between pO2 measurements and FDG uptake but good correlation with 18F-FMISO uptake. No correlation was found between FDG and 18F-FMISO uptake suggesting different tumour uptake mechanisms and characteristics [147, 148]. Another study in head and neck cancer showed the potential role of pre-therapy 18F-FMISO-PET imaging as an independent prognostic marker and that post-therapy changes in the uptake of 18F-FMISO-PET may predict disease free and overall survival [149]. Although 18F-FMISO has been studied extensively for imaging tumour hypoxia, its widespread application is limited by slow tumour-specific accumulation and nonspecific washout.
In an attempt to overcome the disadvantages of 18F-FMISO, second-generation 2-nitroimidazole tracers like 18F-fluoroazomycin arabinoside (18F-FAZA), 18F-fluoroerythronitroimidazole (18F-FETNIM) and 18F-tri-fluoroetanidazole (18F-FETA) were developed which showed better clearance and hydrophilicity characteristics. Preclinical studies have compared 18F-FMISO and 18F-FAZA in tumour xenograft models and found that 18F-FAZA has better pharmacokinetics than 18F-FMISO with higher tumour-to-background and tumour-to-muscle and tumour-to-blood ratios [150, 151]. Clinical studies evaluating the role of 18F-FAZA imaging in identifying tumour hypoxia in head and neck cancer have found it to have a potential role in dose painting for radiotherapy planning [152].
Third-generation hypoxia tracers such as 18F-flortanidazole (18F-HX4) have been developed with a 1,2,3-anti-triazole moiety that makes it more hydrophilic than 18F-FMISO [153]. It is found to have tumour-to-reference tissue values similar to 18F-FMISO at relatively early time points and hence a potential advantage of shorter acquisition times. It has also been evaluated in a preclinical rhabdomyosarcoma tumour model, and the uptake was confirmed to be dependent on tumour oxygenation status. Phase I clinical studies have demonstrated that hypoxia imaging using 18F-HX4 is feasible and nontoxic [154]. A recent comparative study in preclinical animal models showed a clear relationship between the immunohistochemical staining for perfusion, hypoxia and carbonic anhydrase IX and the level of uptake of 18F-FMISO, 18F-FAZA and 18F-HX4. It has been shown that both the 18F-FAZA- and 18F-FMISO-based PET tumour hypoxia uptake for patients in clinical studies have prognostic potential [155].
Other tracers for hypoxia imaging include 64Cu-bis(thiosemicarbazone) complexes (64Cu-ATSM and 64Cu-ATSE). Similarly 64Cu(II)-ATSM has shown promising results in studying tumour hypoxia. Being a neutral lipophilic molecule, it has high membrane permeability, and after cellular uptake, it is converted to [Cu(I)-ATSM] which is negatively charged in hypoxic cells and is trapped [156, 157]. Preclinical studies in R3230 mammary adenocarcinomas, fibrosarcomas and 9L gliomas have shown correlations of 64Cu-ATSM PET hypoxia imaging with other hypoxia markers such as EF5, pimonidazole and CA IX [158]. Preclinical and clinical studies comparing 64Cu-ATSM with 18F-FMISO have shown that regional distribution of 18F-FMISO at 2 h correlates well with the distribution of 64Cu-ATSM at 10 min or 24 h in 9L gliosarcoma tumours and 64Cu-ATSM has been shown to be a safe radiopharmaceutical for imaging tumour hypoxia in human cancers [159, 160].
17.8 PET Tracers for Imaging Apoptosis
Apoptosis or type I programmed cell death is a hallmark of cancer cells and has been extensively exploited to develop novel drug therapies [161]. The various steps in the process of programmed cell death are triggered by appropriate internal and/or external signals leading to preprogrammed cytoplasmic shrinkage and formation of membrane blebs. The process does not incite any inflammatory response [162]. Both radiation therapy and chemotherapy can induce apoptosis in tumour cells, and the rate and extent of apoptosis can be imaged by PET. This information is therefore of great potential interest in monitoring the efficacy of anticancer treatment [163]. Resistance to apoptosis or programmed cell death, a hallmark of cancer cells, has been exploited to develop novel drug therapies. Apoptosis is triggered by endogenous and exogenous stimuli leading to activation of intrinsic and extrinsic pathways of cell death, respectively. These pathways lead to activation of subsets of proteases such as caspase-3, 6 and 7 which target the intracellular proteins involved in DNA damage repair. These agents binding to cell surface proteases have been used to image apoptosis [164, 165]. Annexin-V is a protein that strongly binds phosphatidylserine residue that is externalised to the outer surface of apoptotic cells and is one of the most important probes used in optical and radionuclide imaging. Radiolabelled caspase tracers have also been recently developed [166].
The main methods for imaging apoptosis have been through targeting phosphatidylserine presentation or caspase activation. Recent advances for apoptosis imaging include radiolabelled caspase-3 substrates and inhibitors and monoclonal antibodies targeted to human annexin-V [167].
Agents binding to cell surface proteases that help dying cells to attract phagocytes have been used to image apoptosis. Annexin-V and its derivatives are extensively studied probes targeting apoptosis. 99mTc-labelled annexin-V was the first tracer used to detect cell death in the blood clots of patients who had atrial fibrillation [168]. The first reported use was in an experimental mouse lymphoma model treated with cyclophosphamide. Compared to the untreated mouse, the treated ones showed a 300 % increase in annexin-V uptake 20 h after chemotherapy. Other newer tracers include 99mTc-N2S2-rh annexin-V, used in the clinical setting of lung cancer and lymphomas. 99mTc-labelled annexin-V has also been applied to testing response to radiotherapy. 99mTc-labelled annexin-V scintigraphy [TAVS] was performed in 11 follicular lymphomas patients, and posttreatment TAVS findings matched with posttreatment cytology in 10 patients, confirming TAVS to be a non-invasive imaging modality to detect in vivo apoptosis following radiotherapy [169]. Another annexin-V-labelled tracer is 124I-annexin-V (124I-Anx5) which has been investigated for studying Fas-mediated hepatic cell death in BDF-1 mice using PET. An alternative to annexin-based probes for imaging apoptosis-targeting peptide-1 (ApoPep-1), a hexapeptide that binds to the histone H1 protein in the nucleus, was labelled with 131I to study the biodistribution in normal rats and labelled with 124I for the detection of apoptosis in A549 cell tumours in nude mice [170].
Another molecule which has been extensively studied for PET-based apoptosis imaging is caspase-3. One of the first caspase probes investigated for apoptosis imaging was 131I-labelled benzyloxycarbonyl-Val-Ala-DL-Asp(O-methyl)-fluoromethyl ketone (Z-VAD-fmk) which is a pan-caspase inhibitor. It was studied in Morris hepatoma cells (MH3924Atk8), which showed expression of the herpes simplex virus thymidine kinase (HSVtk) gene. Ganciclovir-induced apoptosis in these cells showed a twofold increase in 131I-Z-VAD-fmk uptake at the end of treatment [171, 172]. Other potential tracers are isatin sulfonamide analogue -based PET probes such as 18F-WC-II-89 and 18F-ICMT-11. 18F-WC-II-89 using micro-PET imaging has been used for studying caspase-3 inside the cell. Preclinical studies have evaluated the role of 18F-ICMT-11 as a caspase-3 specific PET imaging radiotracer and have shown its potential for the assessment of tumour apoptosis in anticancer drug development and the monitoring of early responses to therapy [171]. Though the isatin-based PET probes have shown promising results in imaging of apoptosis, the specificity of these tracers needs to be validated in in vivo models as most of the studies are in a preclinical setting and need validation in a clinical setting [173].
Other radiolabelled imaging targets which have tested in preclinical studies include 99mTc-labelled C2A for studying apoptosis induced by paclitaxel treatment in lung carcinoma and 18F-ML-10-targeted amphipathic apoptosis markers (ApoSense – targeting the cell membrane of apoptotic cells) have been used for clinical imaging and have progressed to phase I/II clinical trials [174, 175].
17.9 PET Tracers for Imaging Tumour Cell Proliferation
Upregulation of cellular proliferation is another hallmark of malignant transformation. PET imaging has played a significant role in imaging cellular proliferation and assessment of therapeutic interventions. One of the first PET radiotracers used for imaging cellular proliferation in tumours was 11C-thymidine [176]. Thymidine is a native nucleoside and is integrated into deoxyribonucleic acids to form DNA. It is taken up by the nucleoside transporters present in the cellular membranes. Once it enters the cell, the enzyme thymidine kinase 1 (TK1) phosphorylates it to thymidine monophosphate. Overexpression of the enzyme TK1 is commonly seen in proliferating tumours and forms the basis of thymidine-based radiolabelled imaging. However, the short 20 min half-life of 11C is the main limiting factor for use of 11C-thymidine in routine clinical practice. Hence, a variety of alternative radiolabelled thymidine tracers have been developed; these include 18F-labelled analogues, 3′-deoxy-3′-18F-fluorothymidine (18F-FLT) and 1-(2′-deoxy-2′-18F-fluoro-β-d-arabinofuranosyl) thymine (18F-FMAU) [177]. Once taken up by the cell, 18F-FLT is phosphorylated by TK1 to 18F-FLT monophosphate and further to 18F-FLT triphosphonate by nucleotide diphosphate kinase, which does not get assimilated into the growing DNA chain as the 3′-position is substituted by 18F and hence undergoes intracellular trapping. Intracellular 18F-FLT retention is quantified and used for measuring the cellular TK1 activity and is an indirect measure of the cellular proliferation rate [178]. It has been shown that the uptake of 18F-FLT increases with increasing TK1 activity in human tumour cell lines, and this uptake was validated with an independent measure of DNA synthesis in tissue. The protein Ki-67 which is a histopathological marker of cellular proliferation, identified by MIB-1 antibody staining, correlates with the level of 18F-FLT uptake measured by PET. This forms the basis of its use as a surrogate marker as an early quantitative measure of drug-induced changes in cellular proliferation [179, 180].
Several studies have shown the promise of 18F-FLT in in vivo imaging, one such example is non-invasive in vitro measurement of growth inhibition of tumour cells caused by a novel histone deacetylase inhibitor (LAQ824) in HCT-116 colon carcinoma xenografts [181]. Several studies concluded that 18F-FLT uptake correlated with histopathological Ki-67 expression and was identified to be an indirect measure of tumour proliferation in non-small-cell lung cancer [180] (Fig. 17.5). Similar results were seen in newly diagnosed/recurrent high-grade gliomas, and 18F-FLT was found to be more sensitive than FDG for detection of tumours in this setting. Also 18F-FLT correlated better with Ki-67 proliferation index and was found to be a better predictor of tumour progression and survival [182]. A clinical study in patients with primary/metastatic breast cancer treated with chemotherapy or hormonal therapy and imaged with 18F-FLT and FDG before, 2 weeks after therapy and at the end of treatment or after 1 year if the therapy was not terminated, revealed that the treatment-induced changes were consistent in both the tracer imaging studies. However, the changes in serum tumour markers correlated more strongly with 18F-FLT uptake than with FDG uptake, and 2-week 18F-FLT uptake correlated with long-term treatment efficacy [183]. Similar results were found in a study reported by Kenny et al. in stage II–IV breast cancer. They concluded that 18F-FLT-PET imaging can predict therapy response to 5-fluorouracil, epirubicin and cyclophosphamide 1 week after initiation of the therapy [184]. Results have been reproduced in several clinical studies in a variety of tumours treated with single or combination therapies. The uptake of 18F-FLT of tumours is dependent on the TK1 activity. Therapy-induced activation of salvage pathways and nucleoside transporter expression also determines the 18F-FLT uptake [185, 186]. Hence drugs such as cytostatic agents which cause cell cycle arrest in the S-phase may increase 18F-FLT uptake [187]. Similarly, agents blocking the endogenous pathway can lead to upregulation of the salvage pathway and increase tumour 18F-FLT uptake. Agents that block both the pathways lead to reduction in 18F-FLT uptake [188]. Despite the promising preclinical and clinical data, limitations are noted in 18F-FLT imaging such as the complex metabolism of 18F-FLT, heterogeneous uptake in tumour tissue, reduced sensitivity in tumours having low expression of TK1 and high background activity in bone marrow and hepatic parenchyma making it more difficult to use in these regions. The clinical utilisation for imaging response of primary and metastatic tumour lesions to therapy therefore remains unclear [189–191] (Table 17.1).