Figure 16.1.1
Complete placenta previa. A: Sagittal midline view of the lower uterus performed transabdominally demonstrates the placenta (PL) completely covering the cervix (CX). B: Sagittal midline view of the lower uterus performed transvaginally on another patient demonstrates the placenta (PL) completely covering the cervix (CX).
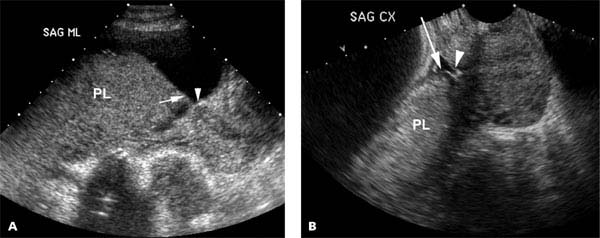
Figure 16.1.2
Marginal placenta previa. Sagittal views of the cervix and lower uterine segment done transabdominally (A) and transvaginally (B) demonstrate the placenta (PL) with its edge (arrow) extending over part of the cervix, ending close to the internal cervical os (arrowhead).
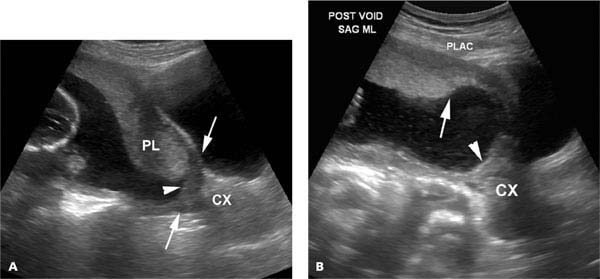
Figure 16.1.3
Pseudo-previa caused by an overly full bladder. A: Sagittal view of the uterus through a distended maternal bladder demonstrates the edge of the placenta close to what appears to be the internal os (arrowhead) of the cervix (CX). B: The woman partially emptied her bladder, after which a sagittal view of the lower segment demonstrates that the placental edge (arrow) does not extend down to the internal os (arrowhead) of the cervix (CX). What had previously appeared to be the cervix were the anterior and posterior walls of the lower uterine segment (arrows in A) pressed in apposition to one another by the overly full maternal bladder.

Figure 16.1.4
Placenta previa demonstrated by manually lifting the fetal head. A: On this sagittal view of the lower uterine segment, the fetal head (HD) casts an acoustic shadow (SH) that obscures the posterior lower uterine segment and a part of the cervix (arrows). A small echogenic structure (arrowhead) that extends caudal to the shadow is suspicious, but not definitive, for a marginal placenta previa. B: Sagittal view of the lower uterine segment after manually lifting the fetal head definitively demonstrates a marginal placenta previa, with the placental edge (long arrow) partially covering the cervix (short arrows).
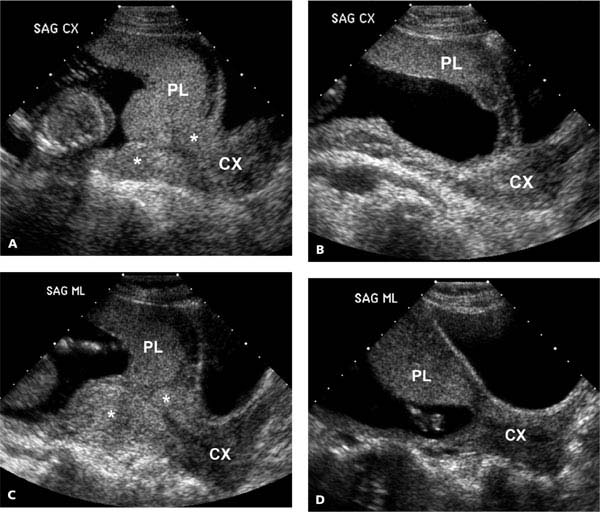
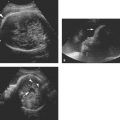
Figure 16.1.5
Lower uterine segment contraction does not permit diagnosis of placenta previa: A: Sagittal midline view of the lower uterus demonstrates a contraction (*’s) in the lower uterine segment. The placenta (PL) appears to overlie the cervix (CX). B: After the contraction resolves it is seen to end well above the cervix. C: Sagittal midline view of the lower uterus in another patient demonstrates a contraction (*’s) in the lower uterine segment. The placenta (PL) appears to overlie the cervix (CX), similar to the appearance in the patient above. D: After the contraction resolves the placenta is seen to cover a portion of the cervix, indicating a marginal previa.
16.2. Placental Abruption
Description and Clinical Features
Placental abruption refers to premature detachment of part or all of the placenta from the uterine wall before delivery of the fetus. The mother often presents clinically with pain and bleeding, but may be asymptomatic. Abruption can lead to fetal damage or death from hypoxia or exsanguination, and hence rapid and accurate diagnosis of abruption can be critical to pregnancy management.
Sonography
Ultrasound does not detect the placental separation itself, but rather can identify a hematoma that might be present with the abruption. The hematoma may be beneath the chorionic membrane (Figure 16.2.1) separate from the placenta or retroplacental (Figure 16.2.2). Less frequently, it is preplacental (Figure 16.2.3). Hematomas vary in appearance, in that they may appear solid or complex and the solid component may be hypo- or hyperechoic relative to the placenta. If the hematoma is isoechoic to the placenta, color Doppler may aid in its detection (Figure 16.2.4), because the hematoma should be avascular while the placenta is vascular.
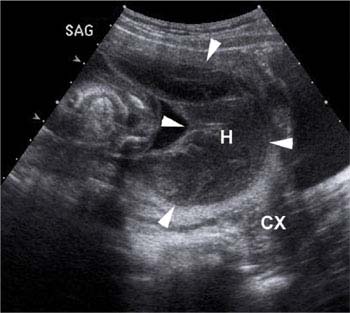
Figure 16.2.1
Placental abruption with large subchorionic hematoma. Sagittal image of lower uterine segment and cervix (CX) showing a large hypoechoic hematoma (H, arrowheads) beneath the chorion, extending across the cervix.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


