Figure 17.1.1
Cervical length measurement. A: Transabdominal measurement (calipers) when the internal os (arrow) is closed (i.e., no funneling). B: Transvaginal measurement (calipers) when the internal os (long arrow) is open and there is U-shaped funneling (short arrow). C: Transvaginal measurement (calipers) when the internal os (long arrow) is open and there is V-shaped funneling (short arrow).

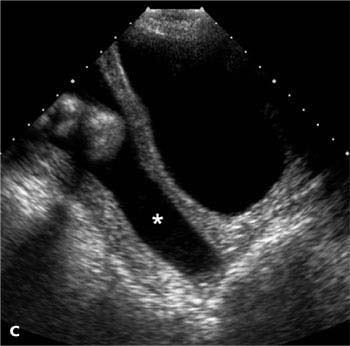
Figure 17.1.2
Incompetent cervix. A: Transvaginal view of the cervix demonstrates a short cervix, measuring 1.9 cm in length, with no funneling. B: Transvaginal view of the cervix (in another case) demonstrates funneling (*), with the length of the residual closed cervix measuring 1.18 cm (calipers). C: Transabdominal view of the cervix (in a third case) demonstrates dilatation of the entire cervical canal (*), with no residual closed cervix.
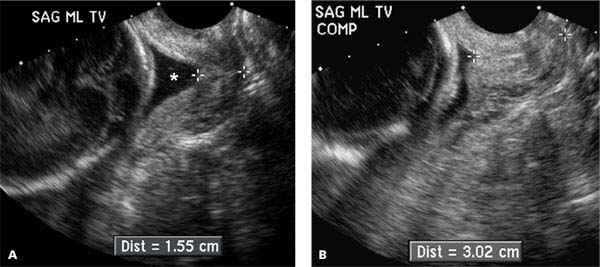
Figure 17.1.3
Transvaginal transducer pressure closing an open cervix. A: Transvaginal sonogram demonstrates cervical funneling (*), with the length (calipers) of the residual closed cervix measuring 1.55 cm. B: When the cervix is compressed (COMP) by the transvaginal transducer, funneling disappears and the length (calipers) of the apparently closed cervix increases to 3.02 cm.
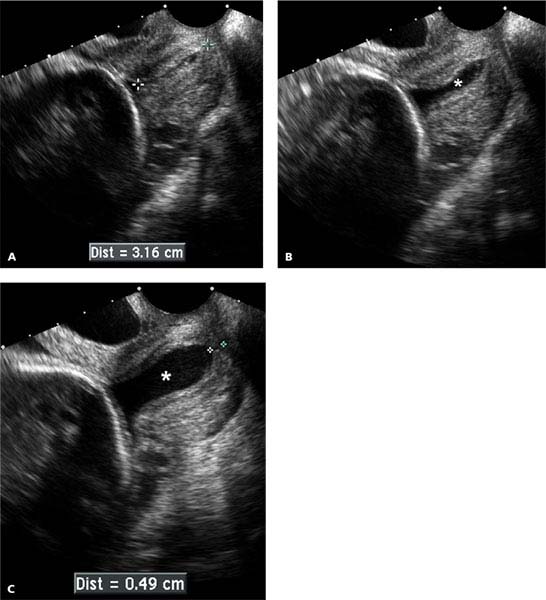
Figure 17.1.4
Spontaneously changing cervix. A: Sagittal transvaginal view of the cervix demonstrates a normal appearing cervix measuring 3.16 cm in length. B: Approximately 20 seconds later, the cervical canal (*) is moderately dilated along its entire length. C: After another 20 seconds, the cervix has dilated further, with the residual closed cervix measuring only 0.49 cm in length.
The length and shape of the cervix may change during the course of the sonogram. This can occur spontaneously (Figure 17.1.4) or may be elicited by manual pressure on the uterine fundus (Figure 17.1.5). In either case, the likelihood of preterm delivery correlates with the shortest length of the cervix during the sonogram.
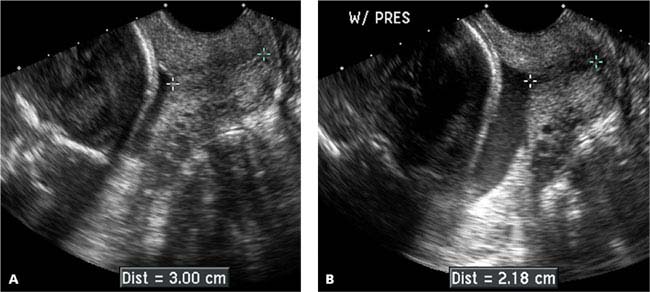
Figure 17.1.5
Cervix dilating with fundal pressure. A: Sagittal transvaginal view of the cervix demonstrates a normal appearing cervix measuring 3.00 cm in length. B: With manual pressure on the uterine fundus (W/ PRES), the cervix shortened to 2.18 cm in length.
17.2. Fibroids in Pregnancy
Description and Clinical Features
Fibroids are common benign myometrial tumors. They are often asymptomatic during pregnancy. In some cases, however, they can lead to pregnancy complications, including the following:
Pregnancy loss: The risk of pregnancy failure is elevated in the presence of fibroids.
Pain: Fibroids will, at times, cause considerable pain during pregnancy. This may be due to the tendency of fibroids to grow during pregnancy, because fibroid growth is often hormonally dependent. The pain is especially severe when a growing fibroid outstrips its blood supply and necroses centrally, a process called “degeneration”.
Obstruction of vaginal delivery: A large lower segment or cervical fibroid may obstruct vaginal delivery.
Placental problems: When the placenta implants on a fibroid, there is increased risk of abruption or intrauterine growth restriction.
Sonography
A fibroid typically appears as a focal uterine mass. It may bulge the outer uterine contour (Figure 17.2.1) and/or indent the gestational sac (Figure 17.2.2). If it is large and situated in the lower uterine segment (Figure 17.2.3), it can interfere with vaginal delivery. The presence of anechoic areas within a fibroid suggests that it has undergone degeneration (Figure 17.2.4).
In some cases, a uterine contraction can have a sonographic appearance somewhat similar to that of a fibroid. Differentiating features include the following:
A fibroid usually has distinct margins whereas a contraction appears as a focal area of myometrial thickening that blends into the adjacent myometrium (Figure 17.2.5).
A fibroid may bulge the outer contour of the uterus, whereas a contraction generally does not.
A fibroid has an unchanging appearance during the entire ultrasound examination, whereas a contraction generally resolves within 10–15 minutes.
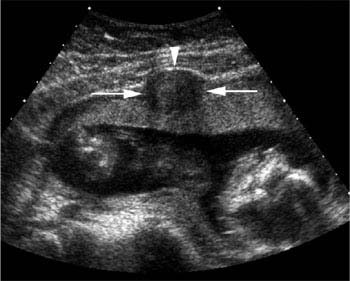
Figure 17.2.1
Uterine fibroid distorting the external contour of the gravid uterus. A fibroid (arrows) is seen as a well-defined hypoechoic mass that bulges the anterior contour of the uterus (arrowhead). The fibroid does not indent the gestational sac.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


