A pneumothorax is a pathologic accumulation of air in the pleural space which, because of the intrinsic elasticity of the lung, leads to separation of the visceral pleura from the parietal pleura.
The various causes of pneumothorax are summarized in ▶Table 11.1. Spontaneous pneumothorax is differentiated from traumatic, including iatrogenic, pneumothorax.
Small pneumothoraces are often asymptomatic or cause sudden chest pain. Larger pneumothoraces may additionally give rise to dyspnea. A small pneumothorax usually resolves spontaneously within a few days and in general requires no treatment but must be monitored. More rapid absorption of the pleural air is achieved through oxygen insufflation. A chest tube is needed for larger pneumothoraces.
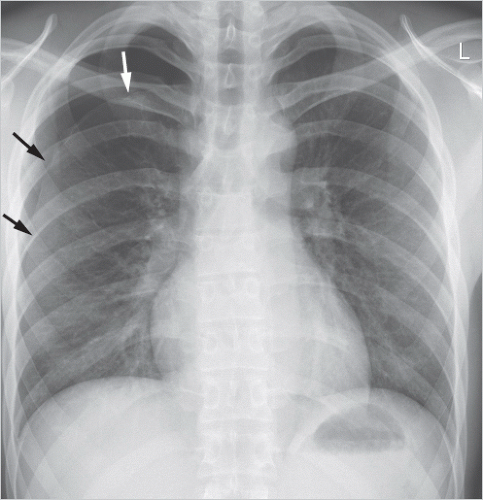
Tension pneumothorax is a special form of pneumothorax (▶Fig. 11.1) in which a valve mechanism caused by the air leak in the visceral pleura allows air to escape from the lung into the pleural space in inspiration but not to return to the lung in expiration. This leads to a progressive pressure increase in the affected hemithorax. Mediastinal displacement toward the unaffected side and a low-riding diaphragm on the affected side are seen on chest radiography. Clinically, there is rapid onset of hypotension, tachycardia, dyspnea, and cyanosis. This dramatic situation stems from several pathophysiologic components4:
Catamenial pneumothorax (in thoracic endometriosis)
Traumatic
Penetrating chest trauma
Displaced rib fracture with rupture of the visceral pleura
Iatrogenic
Transthoracic lung biopsy
Placement of a central venous catheter (subclavian vein)
Thoracentesis
Transbronchial lung biopsy
Pleural biopsy
Positive pressure ventilation
Chest operations
Loss of ipsilateral, negative intrapleural pressure.
Mediastinal displacement to the contralateral side with compression of the intrathoracic superior vena cava and kinking at the transition of the inferior vena cava to the right atrium.
Reduced venous blood return to the heart because of the two aforementioned mechanisms, in turn giving rise to right heart failure.
Onset of atelectasis with an ensuing increase in the pulmonary shunt volume, leading to hypoxemia, which may result in depression of the respiratory center.
Emergency pressure relief of the affected hemithorax through chest tube placement is needed for newly diagnosed tension pneumothorax. Immediate puncture of the pleural space with an adequately long cannula may help bridge the time until a definitive treatment with chest tube is possible.
11.1.1 Imaging Findings
The radiographic findings of pneumothorax will depend on the imaging position (▶Table 11.2).
The most important criterion for a standing radiograph is the ability to identify the visceral pleura, which has separated from the parietal pleura, as a fine linear opacity (▶Fig. 11.3). The space between this line and the chest wall is a more radiolucent and, in general, avascular area (exception: pneumothorax presenting as a backdrop anterior or posterior to the fully inflated lung lobe). Lung adhesions to the chest wall may occur.
Fig. 11.1 Tension pneumothorax. Radiographs. (a) Baseline findings with atelectasis of the right lung (arrow), mediastinal displacement to the left and prominent pulmonary trunk as sign of right heart strain (arrowhead). (b) Normalization of findings following chest tube placement.
Note
Expiratory radiographs as customarily obtained in the past for diagnostic imaging of pneumothorax have no relevant diagnostic advantages over those obtained in inspiration.5,6 Furthermore, expiratory radiographs hamper diagnostic exploration of pulmonary opacities (e.g., lung contusions in suspected traumatic pneumothorax) and make it harder to compare previous or follow-up inspiratory images. Therefore, inspiratory radiographs should, generally, be used for diagnostic imaging of pneumothorax.
Because the patient is lying down, supine radiographs result in an anterior pleural air collection that hampers direct detection of a visceral pleural line since often the lung abuts the lateral chest wall. Hence, diagnosis is based on indirect signs of air in the pleural space as presented in ▶Table 11.2.
Table 11.2 Projection radiography findings of pneumothorax
Increased radiolucency between lung and chest wall
Increased radiolucency of one lung
Vasculature cannot be identified between the lung and chest wall
More radiolucent, broader and lower costophrenic angle (deep sulcus sign, ▶Fig. 11.2)
Fig. 11.2 Pneumothorax. Radiograph, supine position. Compared with the right side, increased radiolucency of the left lung, more clearly delineated left heart border (arrowhead) and more radiolucent as well as lower left costophrenic angle-deep sulcus sign (arrows). Besides, chest tube on the left.
Computed tomography (CT) has greater sensitivity than radiography for diagnosis of smaller pneumothoraces. It is even able to reliably detect pneumothorax in cases where the radiograph was inconclusive, e.g., because of chest wall emphysema. CT often provides additional information on the etiology of spontaneous pneumothorax and in many cases contributes to diagnosis and differential diagnosis of pulmonary causes (▶Fig. 11.4). The indications for CT are listed in ▶Table 11.3.
11.1.2 Differential Diagnosis
In the presence of bullous pulmonary emphysema, it may be difficult to reliably differentiate between an emphysematous bulla and pneumothorax since both entities manifest as an avascular space. CT is useful in such cases; to that effect, the visceral pleura should be identified to differentiate between a pleural (pneumothorax) and subpleural (emphysematous bulla) location of the air.
Fig. 11.3 Spontaneous pneumothorax. Radiograph. Visible pleural line, consistent with the visceral pleura (arrows). Between the pleural line and chest wall a more radiolucent and avascular space.
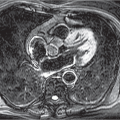
Fig. 11.4 Spontaneous pneumothorax. Examples of causes to be diagnosed on CT. (a) Right apical emphysematous bullae (same patient as in ▶Fig. 11.3). (b) Catamenial pneumothorax with pleural-based endometriosis nodule (arrow). Besides, minor pleural effusion.
Skin folds can mimic pneumothorax on supine radiographs, less commonly on standing radiographs (▶Fig. 11.5). The key criteria for this pseudopneumothorax are vascular structures between the presumed pleural line and chest wall as well as disappearance of the presumed pleural line in the middle of the lung or its extension beyond the border of the hemithorax.
CT is generally not indicated for first-time pneumothorax; it can be useful for recurrent pneumothorax or clinically suspected underlying pulmonary disease that cannot be identified on a radiograph
Secondary and catamenial pneumothorax
CT is generally not indicated for first-time pneumothorax; it can be useful for recurrent pneumothorax, for persistent air leak with drainage or for preoperative management
Traumatic pneumothorax
CT is usually performed in any case as part of the diagnostic trauma work-up; however, in the presence of isolated rib fractures, pneumothorax requiring treatment can be reliably excluded with a radiograph
Fig. 11.5 Left pseudopneumothorax (skin fold). Radiograph, supine position. Line running in caudal direction superior to the diaphragmatic contour (arrows), mimicking a pleural line. Besides, chest tube after right lower lobe resection.
11.2 Pleural Effusion
Pleural effusions are caused by many pathologic conditions (▶Table 11.4). A distinction is made between transudates and exudates on the basis of their origin. Transudates stem from passive filtration of serous fluid into the pleural space, whereas exudates derive from secretion of protein-rich fluid. This distinction can be made through simple laboratory tests of pleural fluid. The effusion is classified as an exudate if at least one of the following criteria is met8:
A pleural fluid-to-serum protein ratio greater than 0.5.
A pleural fluid-to-serum lactate dehydrogenase level (LDH) ratio greater than 0.6.
A pleural fluid LDH of more than two-thirds of maximum normal serum LDH.
Likewise, other fluids (e.g., blood, pus, or chyle) manifest as pleural effusion on imaging.
Cross-sectional imaging, particularly ultrasound, is most sensitive for detection of pleural effusion. Lateral radiographs demonstrate pleural effusions larger than 50 mL, which are initially seen as opacification of the posterior costodiaphragmatic angle. Pleural effusions larger than 100 mL are visible on posteroanterior (PA) radiographs in the lateral costodiaphragmatic angle. Because of geometric projection conditions, pleural effusions appear meniscus-shaped in standing radiographs (▶Fig. 11.6).
In supine radiographs, pleural effusion is located posterior to the lungs and is distributed more or less evenly in the chest cavity, thus causing only diffusely reduced radiolucency of the affected hemithorax. Even several hundred milliliters of pleural effusion can be overlooked in supine radiographs.
Congestive left heart failure, pneumonia, pulmonary embolism
Elevated intravascular pressure in the pleura
Congestive left heart failure Congestive right heart failure
Superior vena cava syndrome
Elevated capillary permeability
Pleuritis
Elevated protein content of pleural fluid
Pulmonary edema, hemothorax
Reduced pressure in the pleural space
Atelectasis
Increased fluid in the peritoneum
Ascites, peritoneal dialysis
Rupture of the thoracic duct
Chylothorax
Rupture of thoracic blood vessels
Hematothorax
Reduced pleural fluid absorption
Obstruction of parietal pleura lymph drainage
Malignant tumor, lymphoma
Elevated systemic venous pressure
Congestive right heart failure, superior vena cava syndrome
Fig. 11.6 Right pleural effusion. Radiograph. Meniscus-shaped opacity of the right lateral costophrenic angle.
A subpulmonary pleural effusion occasionally mimics a high-riding diaphragm and can be suspected if the highest point of the diaphragm is located lateral to its middle. Isolated interlobular effusions sometimes present as well-defined oval pulmonary opacities on radiography. These are known as “vanishing tumors” since they tend to migrate and disappear within a few days.
11.3 Pleural Empyema
Pleural empyema is an infection of the pleural cavity usually manifesting as pathologic pleural fluid collection. This is often caused by pneumonia, with the infection spreading secondarily into the pleural space, giving rise to an independent disease process. Less commonly, pathogens use other portals of entry, for example, a perforated lung tumor in the pleural space, following chest injury or as a complication of a surgical procedure. Pleural empyema is distinguished from a noninfected pleural effusion through laboratory analysis of the pleural fluid.10 A summary of the criteria used to differentiate between pleural empyema and noninfected pleural effusion is given in ▶Table 11.5. The most commonly implicated pathogens are gram-negative bacteria as well as Staphylococcus aureus and anaerobes.11 Tuberculosis, too, can give rise to pleural empyema. The continuous development of a chest wall abscess from a pleural empyema is known as “empyema necessitatis” (or “empyema necessitans”), which is often but not exclusively seen in mycobacterial infection.
Exudative phase: In the visceral pleura, the inflammatory process leads to increased capillary permeability, and consecutively to exudation of protein-rich fluid into the pleural space causing an exudative pleural effusion. There is still no sign of pleural thickening.
Fibrinopurulent phase: In the later course, inflammatory cells and neutrophils migrate into the pleural fluid, and fibrin is deposited on the pleural surfaces, causing thickening of the visceral and parietal pleura.
Organizing phase: Fibroblast activity and capillary neogenesis lead to collagen deposition and ingrowth of granulation tissue on the pleural surfaces, and subsequent pleural fibrosis. This reaction can be very intense and lead to development of extensive pleural thickening.
Treatment is tailored to the cause and stage of pleural empyema. The underlying cause is treated whenever possible. The specific treatment for pleural empyema in the exudative phase usually consists of chest tube placement and appropriate antibiotic treatment. More advanced pleural empyema, in particular in the presence of pleural thickening, requires surgical decortication.
Table 11.5 Differentiation between pleural empyema and noninfected pleural effusion in a fluid sample obtained from thoracentesis.10 One positive criterion suffices for diagnosis of pleural empyema