Abstract
Pleural effusion, a common observation with a variety of causes, is a very nonspecific finding that requires a careful search for associated findings and clinical correlation. Congestive heart failure is one of the most common causes of pleural effusion that is diagnosed by combining the patterns of cardiac enlargement with increased size of the pulmonary vessels and reticular interstitial opacities that may progress to diffuse bilateral airspace opacities. Other associated findings or clinical history may provide clues for the diagnosis of trauma, empyema, metastases, or other systemic diseases. Pleural effusion is always abnormal and requires a specific diagnosis.
Keywords
abdominal diseases, collagen vascular diseases, drug reactions, heart failure, pleural tumors, thoracic trauma
Questions
- 1.
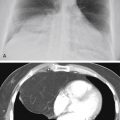
The most likely diagnosis in the case illustrated in Fig. 4.1 is:
- a.
Necrotizing pneumonia with empyema.
- b.
Tuberculosis.
- c.
Lung cancer.
- d.
Mesothelioma.
- e.
Metastases.

Fig. 4.1
- a.
- 2.
The most likely diagnosis in the case illustrated in Fig. 4.2, A and B, is:
- a.
Right lower-lobe pneumonia.
- b.
Pulmonary embolism.
- c.
Subphrenic abscess.
- d.
Lymphoma.
- e.
Diaphragmatic hernia.

Fig. 4.2
- a.
Discussion
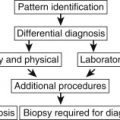
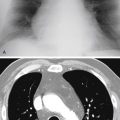
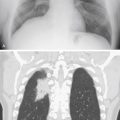
Pleural effusions may produce blunting of a costophrenic angle (see Fig 4.1 ), apparent elevation of the diaphragm (see Fig 4.2, A ), peripheral homogeneous opacity with a line that parallels the lateral chest wall ( Fig 4.3 ), opacity in interlobar fissures ( Fig 4.4, A-D ), 465 or complete opacification of an entire hemithorax, with a shift of the mediastinum ( Fig 4.5 ). Detection and confirmation are often the first steps in the evaluation of a suspected pleural effusion. Small effusions with opacification of the costophrenic angle may be confirmed by a lateral decubitus examination, with the side of the suspected effusion down. The decubitus examination may show a change in position of the opacity and confirm free-flowing effusion. No change in the opacity may be the result of loculated effusion, pleural scarring, or possibly a pleural mass. Prior chest radiographs indicating that the blunting is a new finding also provide a good indicator of pleural effusion. Loculated effusions are difficult to confirm with chest radiograph, but ultrasound, computed tomography (CT), and even magnetic resonance imaging (MRI) may be used to verify a localized collection of pleural fluid. The differential diagnosis of pleural effusion entails consideration of a long list of entities ( Chart 4.1 ), 465 but the radiologist should not be discouraged. 478 Pleural effusion is sometimes associated with additional radiologic findings that may be very specific, but clinical and laboratory correlation are almost always required to make a specific diagnosis.



- I.
Congestive heart failure 6 , 390
- II.
Thromboembolic disease 660
- III.
Infection
- A.
Bacteria ( Klebsiella pneumoniae , Staphylococcus aureus , Streptococcus pyogenes , Nocardia asteroides , 29 Streptococcus pneumoniae [Diplococcus] , 578 anaerobic organisms, 324 anthrax, 125 , 648 actinomycosis, 164 other necrotizing bacterial infections)
- B.
Tuberculosis
- C.
Viral (uncommon)
- D.
Mycoplasma (uncommon)
- E.
Fungus (blastomycosis, coccidioidomycosis, 431 histoplasmosis, cryptococcosis 504 [effusion secondary to fungal infection is rare])
- F.
Parasites ( Entamoeba histolytica , 639 Echinococcus , Paragonimus , 260 , 262 malaria)
- G.
Infectious mononucleosis
- A.
- IV.
Neoplasms
- A.
Metastases
- B.
Bronchogenic carcinoma
- C.
Distant (e.g., breast, gastrointestinal, pancreatic)
- D.
Multiple myeloma
- E.
Mesothelioma
- F.
Chest wall—primary bone cancer (e.g., Ewing sarcoma, chondrosarcoma, osteosarcoma, fibrosarcoma)
- G.
Lymphoma 620
- H.
Waldenström macroglobulinemia
- A.
- V.
Collagen vascular disease (autoimmune)
- A.
Systemic lupus erythematosus 632
- B.
- C.
Granulomatosis with polyangitis 4 (formerly Wegener granulomatosis)
- D.
Scleroderma (rare) 19
- A.
- VI.
Trauma
- A.
Chest wall trauma
- B.
Rupture of the esophagus
- C.
Rupture of the thoracic duct
- D.
Laceration of great vessels (e.g., aorta, vena cava, pulmonary veins)
- A.
- VII.
Abdominal diseases
- A.
Pancreatitis
- B.
Pancreatic neoplasms
- C.
Pancreatic pseudocyst
- D.
Pancreatic abscess
- E.
Subphrenic abscess
- F.
Abdominal or retroperitoneal surgery (e.g., renal surgery, splenectomy)
- G.
Urinary tract obstruction with extension of retroperitoneal urine 31
- H.
Ovarian tumors (e.g., Meigs syndrome)
- I.
Cirrhosis of the liver
- J.
Peritoneal dialysis
- K.
Renal disease
- L.
Renal failure
- M.
Acute glomerulonephritis
- N.
Nephrotic syndrome
- O.
Whipple disease
- A.
- VIII.
Diffuse pulmonary diseases
- A.
Lymphangioleiomyomatosis 424 (LAM)
- B.
Asbestosis (rare)
- C.
Usual interstitial pneumonitis (rare)
- D.
Sarcoidosis (reported to be 4% of cases) 635
- A.
- IX.
Drug reactions
- A.
Nitrofurantoin
- B.
Methysergide
- C.
Busulfan
- D.
Procainamide
- E.
Hydralazine
- F.
Isoniazid (INH)
- G.
Phenytoin sodium (Dilantin)
- H.
Propylthiouracil
- I.
Procarbazine
- A.
- X.
Other
- A.
Postmyocardial infarction syndrome (Dressler syndrome) and postpericardiotomy syndrome
- B.
Coagulation defect
- C.
Radiation therapy (very rare) 628
- D.
Idiopathic
- E.
Pleural fistulas (bronchial, gastric, esophageal, subarachnoid) 220 , 638
- F.
Empyema from retropharyngeal and neck abscess
- G.
Empyema in postpneumonectomy space 231
- A.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


