45 Popliteal Block
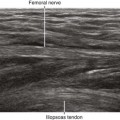
The tibial nerve visibility is best near the knee crease because of the relatively small extremity size. In that location, the typical anatomy is popliteal artery, popliteal vein, and tibial nerve (listed from deep to superficial within a parasagittal plane). The tibial nerve is about twice the size of the common peroneal nerve in terms of cross-sectional area.1 The tibial nerve has a straight course near the middle of the lower extremity, whereas the common peroneal nerve has a more oblique (lateral) course (Table 45-1).
Table 45-1 Characteristics of the Bifurcation of the Sciatic Nerve in the Popliteal Fossa
| Nerve | Common Peroneal Nerve | Tibial Nerve |
|---|---|---|
| Position | Lateral | Medial |
| Posterior (superficial) | Anterior (deep) | |
| Diameter (mm) | 4.0 | 6.5 |
| Course | Oblique | Straight |
| Associated structures | Joins conjoint tendon of biceps femoris distally | Joins popliteal artery and vein distally |
| Echotexture | Less hyperechoic | More hyperechoic |
| Fewer fascicles | More fascicles | |
| Larger fascicles | Smaller fascicles | |
| Response to foot dorsiflexion | Moves anteriorly | Moves posteriorly |
The common peroneal nerve travels distally along the posterior or medial aspect of the conjoint tendon of the biceps femoris near the knee crease. With the foot in neutral position, the common peroneal nerve usually lies slightly closer to the posterior surface of the leg than the tibial nerve.2 Because it is smaller and has fewer fascicles, the common peroneal nerve is more difficult to identify than the tibial nerve.3
Suggested Technique
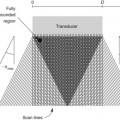
Elevation of the leg and some internal rotation allow imaging of the popliteal fossa from the posterior surface.4 A broad linear transducer (35- to 50-mm footprint, 10 MHz center frequency) is used for most adult patients. The choice of block needle (7- to 9-cm length, 20-22 gauge) is not critical.
Popliteal block is usually performed just distal to the sciatic nerve bifurcation in the popliteal fossa for several reasons. First, the nerves are close to the posterior skin surface. This makes nerve imaging and positioning the needle tip easier. Second, the needle can be aimed at the connective tissue space between the tibial and common peroneal nerves (rather than directly aimed at the sciatic nerve).5 The block is performed where the tibial and common peroneal nerves are about one needle-width apart (about 1 mm). Third, there is a large amount of nerve surface area available for diffusion of local anesthetic to promote clinical block characteristics. The point of sonographic unity is closer to the knee crease than anatomic dissections would suggest because the tibial and common peroneal nerves run next to each other for some distance before visibly separating. The only potential disadvantage to this more distal popliteal block is that the popliteal vessels are closer to the nerves.
Studies have suggested a limited ability of ultrasound to correctly assess circumferential distribution of local anesthetic around peripheral nerves. The reported predictive value of the “doughnut” sign is only about 90% for sciatic nerve blocks.6




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


