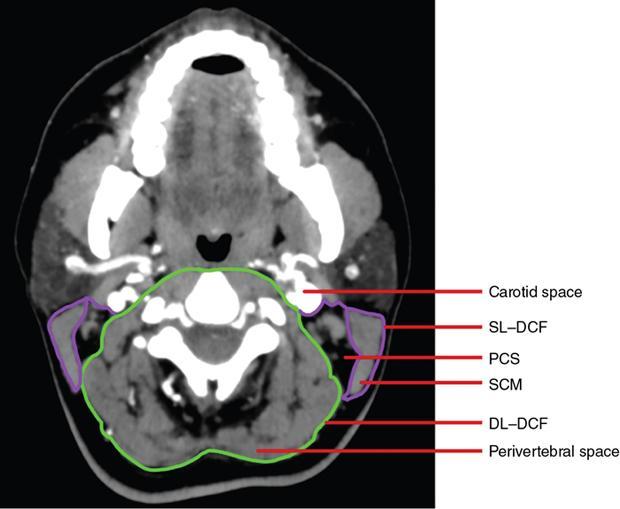
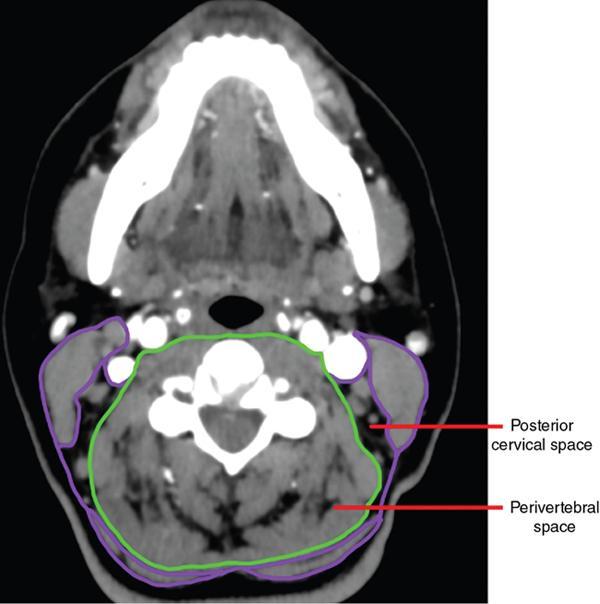
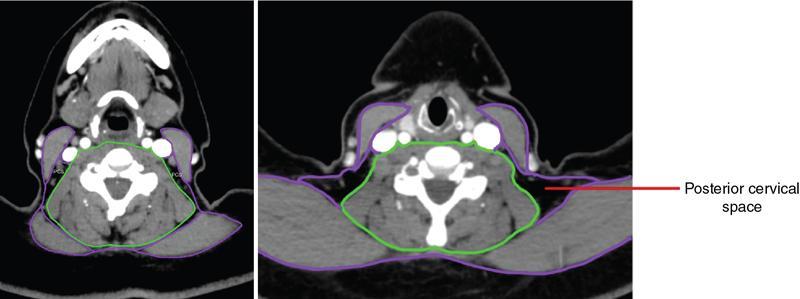
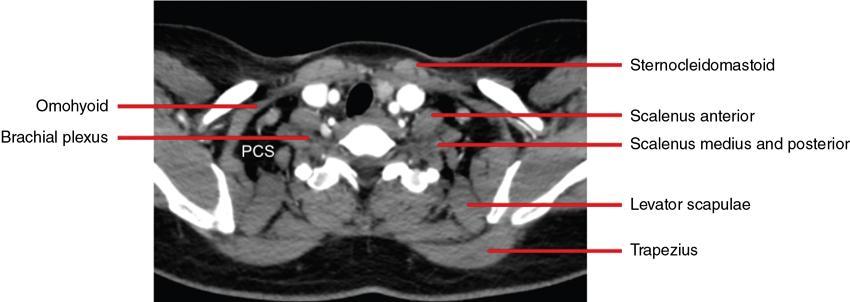
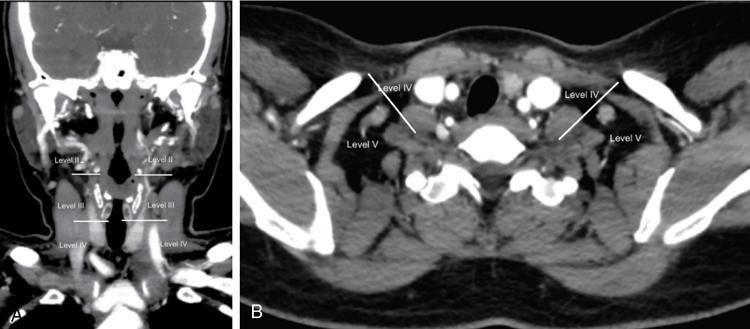
Anita Nagadi The posterior cervical space lies along the posterolateral aspect of the neck and is also commonly referred to as the posterior triangle of the neck by the surgeons. The posterior cervical space extends from the level of the skull base down to the clavicles. This space lies deep to the sternocleidomastoid and trapezius muscles, but superficial to the perivertebral space. The space is small cranially and gradually expands in a caudal direction where it is finally related to the middle third of the clavicle. Superficial to the PCS lie the sternocleidomastoid and trapezius muscles which are lined by the superficial layer of deep cervical fascia (SL–DCF). Along the deeper aspect, the PCS is separated from the perivertebral space by the deep layer of deep cervical fascia (DL–DCF). Anteromedially, the PCS is related to the carotid space which is lined by contributions of all the three layers of the deep cervical fascia. The contents of the PCS are fat, lymph nodes and nerves. Several groups of lymph nodes lie in the posterior cervical region. Those that lie posterior to the posterior border of the sternocleidomastoid are classified as level V lymph nodes. The lymph nodes that lie deep to the sternocleidomastoid are classified as level II to level IV lymph nodes. The craniocaudal landmarks that help separate these levels are the inferior margin of the hyoid and cricoid cartilages. The lymph nodes that lie above the level of the inferior margin of the hyoid cartilage are labelled as level II, those that lie beneath the inferior margin of the cricoid cartilage are labelled as level IV and the ones in between are level III lymph nodes. The main nerves to traverse the posterior cervical space are the spinal accessory nerve (XI) and the dorsal scapular nerve. The distal portions of the brachial plexus also traverse the lower PCS. The spinal accessory nerve runs along the deep surface of the sternocleidomastoid and crosses the posterior cervical space in an oblique direction to run along the deep surface of the trapezius. The trunks of the brachial plexus emerge between the anterior and middle scalene muscles and divide into divisions and cords within the PCS before continuing into the axilla. The dorsal scapular nerve and the cutaneous branches of the cervical plexus also traverse the PCS. The third part of the subclavian artery briefly traverses the inferior aspect of the PCS as it emerges behind the anterior scalene muscle and continues distally to pass over the first rib. The clinicians refer to the PCS as the posterior triangle of the neck bordered by the sternocleidomastoid anteriorly and the trapezius muscle posteriorly. The triangle is further divided by the inferior belly of the omohyoid into a superior occipital triangle and inferior subclavian triangle (Figs 3.20.1–3.20.5). KEY POINTS FROM ANATOMY
3.20: Posterior cervical space
Introduction
Extent and division
Boundaries
Relations
Contents
Key points from anatomy
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Posterior cervical space