Fig. 6.1
Stress radiographic measurement of a posterior cruciate ligament and posterolateral corner of the injured knee. (a) Demonstrates posterior subluxation of the tibia relative to the femur at approximately 90° of knee flexion. (b) Demonstrates normal relationship of the femur and tibia in the patient’s uninjured normal knee
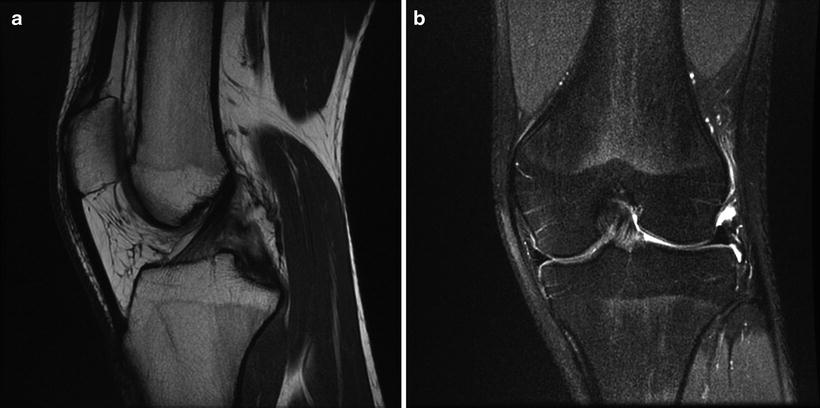
Fig. 6.2
(a) Magnetic resonance imaging revealed full-thickness tear of the posterior cruciate ligament seen in the midportion of the ligament primarily extending to the insertion with no detachment of the insertion. (b) MRI of the posterolateral corner revealed edema and some tearing of the posterolateral capsular structures, although no gross disruption of the fibular collateral ligament or popliteus tendon. The remaining structures were intact
Arthroscopy
The patient was taken to the operating room and positioned supine on the fully extended operating table. The examination of the left knee under anesthesia was in agreement with the physical examination outlined above. Arthroscopic examination of the left knee joint revealed the articular cartilage in all three compartments to be intact, medial and lateral menisci to be intact, lateral joint space opening (positive drive thru sign), zone 1–2 posterior cruciate ligament tear, and the anterior cruciate ligament to be intact but exhibiting the sloppy ACL sign consistent with PCL injury [15] (Fig. 6.3a, b).
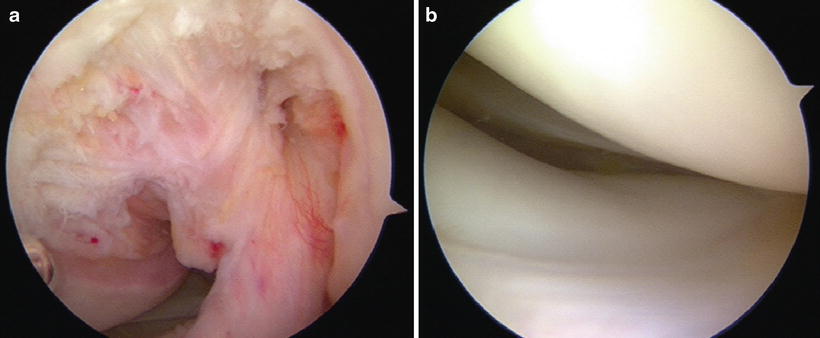
Fig. 6.3
Arthroscopic photographs of the posterior cruciate ligament tear and the posterolateral corner. (a) Arthroscopic evaluation of the PCL revealed a zone 1–2 posterior cruciate ligament tear, with the anterior cruciate ligament to be intact but exhibiting the sloppy ACL sign consistent with PCL injury. (b) Arthroscopic evaluation of the lateral compartment and posterolateral corner revealed lateral joint space opening in the figure four position with a positive drive thru sign consistent with posterolateral instability of the knee
Discussion and Surgical Reconstruction
The patient had a functionally unstable knee indicating the need for surgical reconstruction. Since this was a chronic injury with consistent soft tissue configuration, a single-stage combined posterior cruciate ligament and posterolateral reconstruction was performed. The arthroscopic findings were in agreement with the physical examination findings and the MRI findings of combined posterior cruciate ligament injury and posterolateral corner injury. Combined posterior cruciate ligament reconstruction and posterolateral reconstruction were performed. PCL reconstruction was a transtibial arthroscopic double-bundle reconstruction using Achilles tendon and tibialis anterior allograft tissue using mechanical graft tensioning, and the posterolateral reconstruction was a fibular head-based figure of eight reconstruction using semitendinosus allograft tissue combined with a posterolateral capsular shift procedure and peroneal nerve decompression and neurolysis [36–38] (Fig. 6.4a–d).
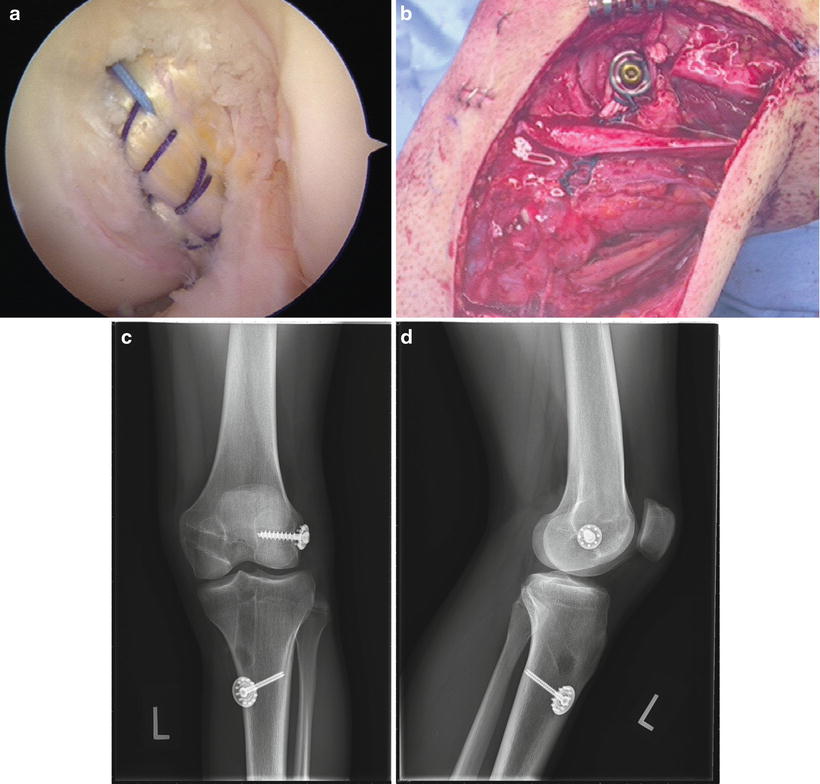
Fig. 6.4
Posterior cruciate ligament and posterolateral reconstruction of the knee. (a) Posterior cruciate ligament reconstruction was performed using a transtibial arthroscopic double-bundle reconstruction with an Achilles tendon allograft for the anterolateral bundle and tibialis anterior allograft for the posteromedial bundle. A mechanical graft-tensioning device was used for graft tensioning. (b) Posterolateral reconstruction was performed using a fibular head-based figure of eight reconstruction with a semitendinosus allograft tendon combined with a posterolateral capsular shift procedure. Peroneal nerve decompression and neurolysis is always performed, and the peroneal nerve is carefully protected throughout the procedure. (c, d) Postoperative anteroposterior and lateral radiographs of the posterior cruciate ligament and posterolateral reconstructed knee demonstrating tunnel and hardware position and orientation
Case 2
History/Physical Exam
A 31-year-old man fell from a height of approximately 5 ft and upon landing twisted his left knee resulting in a left tibiofemoral knee dislocation that was reduced at the scene of the accident. Physical examination in the emergency department revealed neurovascular structures to be intact. Range of motion was restricted secondary to pain. The affected knee had negative tibial step offs and a grade 3 positive posterior drawer at 90° of knee flexion. The posterolateral drawer was positive, and the posteromedial drawer was negative. There was severe varus laxity at zero and 30° of knee flexion with no discernible end point. The Lachman test was positive, and the pivot shift was positive. The dial test was positive at both 30° and 90° of knee flexion. There was no valgus laxity with the medial side being the stable hinge.
Imaging Studies
Plain radiography demonstrated good reduction and alignment of the tibiofemoral and patellofemoral joint. Stress radiography of the knees was not obtained preoperatively due to the severe instability of the left knee.
Magnetic resonance imaging revealed full-thickness complete tears of the posterior and anterior cruciate ligaments (Fig. 6.5a, b). There was increased signal in the proximal medial collateral ligament just distal to its femoral attachment with associated periligamentous edema consistent with a moderate sprain. A tear of the meniscofemoral ligament was also noted. The posteromedial corner structures were intact, as well as the pes tendons.
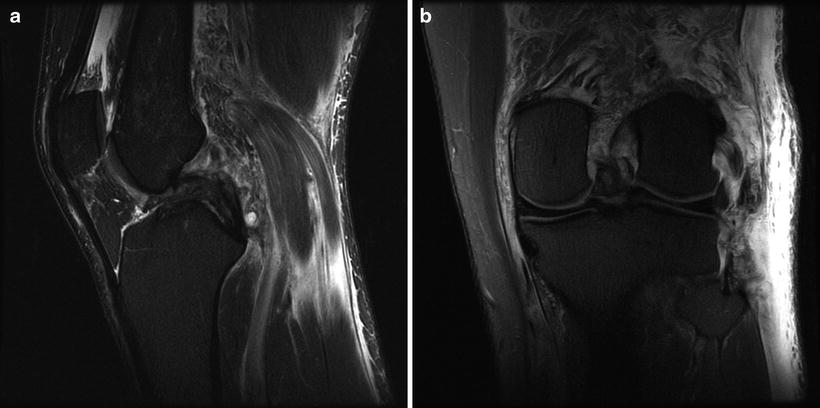
Fig. 6.5
Magnetic resonance imaging studies demonstrating injury to the posterior and anterior cruciate ligament and the posterolateral corner of the left knee. (a) Magnetic resonance imaging revealed full-thickness complete tears of the posterior and anterior cruciate ligaments consistent with the patient’s mechanism of injury, history, and clinical examination. (b) MRI demonstrates increased signal in the proximal medial collateral ligament just distal to its femoral attachment with associated periligamentous edema consistent with a moderate sprain. A tear of the meniscofemoral ligament was also noted. The posteromedial corner structures were intact, as well as the pes tendons. MRI demonstrates that the lateral and posterolateral structures were severely damaged. The conjoined tendon of the biceps femoris and the fibular collateral ligament were completely torn and retracted from their fibular attachments with surrounding edema. There was a near complete tear of the popliteus tendon from its femoral origin. There was a low-grade sprain of the popliteus at the myotendinous junction, with a sprain of the popliteal fibular ligament without complete disruption. There was a lateral capsular avulsion with the iliotibial band intact
The lateral and posterolateral structures were severely damaged (Fig. 6.6a, b). The conjoined tendon of the biceps femoris and the fibular collateral ligament were completely torn and retracted from their fibular attachments with surrounding edema. There was a near complete tear of the popliteus tendon from its femoral origin. There was a low-grade sprain of the popliteus at the myotendinous junction, with a sprain of the popliteal fibular ligament without complete disruption. There was a lateral capsular avulsion with the iliotibial band intact.
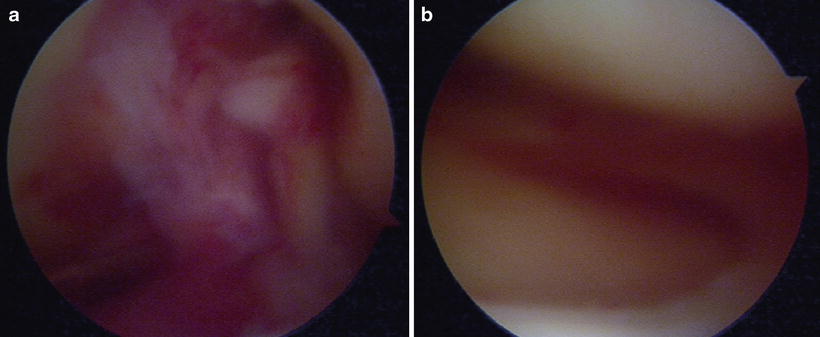
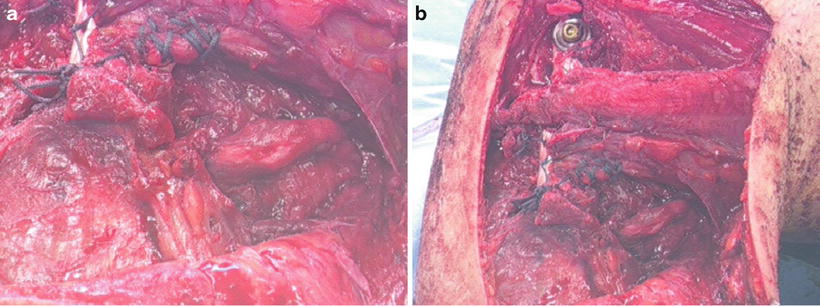
Fig. 6.6
Arthroscopic view of the injured posterior and anterior cruciate ligaments (a) and the injured posterolateral corner structures (b). Note in b the drive thru sign with the knee in the figure four position and the position of the lateral meniscus relative to the femur and tibia
The extensor mechanism, patellofemoral stabilizers, and articular cartilage in the medial, lateral, and patellofemoral compartments were all intact. There was a bone bruise on the medial femoral condyle.
Treatment Decision
The patient had a severe left knee injury with gross instability and severe damage to the lateral and posterolateral structures. The decision was made to proceed with a two-stage approach for surgical treatment of this PCL, ACL, and type C posterolateral multiple-ligament injured knee that was an acute tibiofemoral knee dislocation [39].
Discussion and Surgical Reconstruction
Stage 1 was repair and reconstruction of the lateral posterolateral side/corner structures approximately 10-day post injury when the skin and other soft tissues had stabilized (Fig. 6.7a, b). The patient had been immobilized in a brace locked in full extension with provisional preoperative mobilization. Stage 1 surgery consisted of peroneal nerve decompression and neurolysis, primary repair of all injured lateral and posterolateral structures, and posterolateral reconstruction with a fibular head-based figure of eight reconstruction using semitendinosus allograft tissue combined with a posterolateral capsular shift procedure [36–38]. Stage 2 was an arthroscopic combined posterior and anterior cruciate ligament reconstruction performed 4 weeks after the stage 1 procedure. Posterior cruciate ligament reconstruction was a transtibial arthroscopic single-bundle reconstruction using Achilles tendon allograft tissue, and the anterior cruciate ligament reconstruction was an arthroscopic transtibial femoral tunnel reconstruction using Achilles tendon allograft tissue and mechanical graft tensioning for both the PCL and ACL reconstructions [40, 41] (Fig. 6.8a, b).