, Natasha Sallum1 and Lydia Masako Ferreira1
(1)
Division of Plastic Surgery, Federal University of São Paulo/UNIFESP, São Paulo, Brazil
11.1 Introduction
Cleft lip and palate are the most common causes of facial malformation, with an approximate incidence of 1 in 1250 live births [1, 2]. The high incidence of this malformation is due to the sensitivity of the cells of the face to teratogenic events.
The birth of a child with facial cleft results in a strong emotional reaction by the parents. Very early correction of the defect, even during the same hospital stay as the birth, may be desired by the parents. This treatment is adopted by some surgeons and is seen as a strategy to improve the family’s experience when a child is affected with a facial congenital deformity.
However, most surgeons prefer to delay correction of these defects until the child is at least 3-6 months of age when the structures are larger and more readily identifiable [3].
11.2 Embryology
Understanding of the development of the cleft lip and palate can be obtained from the knowledge of the embryological structures from which the facial bones and soft tissues originate (Table 11.1 and Fig. 11.1).

Table 11.1
Embryological origin of facial bones and soft tissues
Embryological structure | Anatomical area | Anatomical structures |
|---|---|---|
Nasal prominence | Primary palate | Premaxilla |
Anterior septum | ||
Upper lip | ||
Maxillary prominence | Secondary palate | Hard palate (posterior to the incisive foramena) |
Soft palate | ||
Uvula |
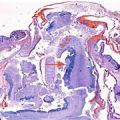
Fig. 11.1
Bilateral cleft lip (preforamen cleft). The photograph shows the embryological differentiation of the structures formed by the primary and secondary palates
11.3 Diagnosis
Except for some posterior palate clefts hidden by a mucosal union between the left and right sides, facial clefts may be diagnosed by prenatal ultrasound. The upper lip and palate can be visualized, and an eventual loss of continuity of the tissues can be detected [4].
11.4 Classification
There are many classifications of face and palate clefts in the literature. One of the most used is the one described by Kernahan [5] that classifies the labial palate clefts using the shape of the letter “Y.” The center of the “Y” is represented by the incisive foramen. A simple classification of the labial palate clefts can be seen as follows (Table 11.2).
Table 11.2
Classification of the labial palate clefts
Cleft | Lip | Complete | Right |
Palate | Incomplete | Left | |
Lip and palate | Bilateral |
The ideal timing for surgical correction of cleft lip and palate is at the following ages:
Primary cleft lip correction: from 3 to 6 months
Primary palatoplasty: from 18 to 24 months, before the development of the speech
Alveolar bone graft: around 12 years old
Rhinoseptoplasty: after 16 years old
Orthognathic surgery: after 16 years old
11.5 Clinical Aspect – Breast Feeding
Most children with cleft lip and/or cleft palate can breastfeed normally, although some may experience difficulties. When the nasal cavity communicates with the oral cavity, there is less negative pressure that is able to be created within the mouth during the infant’s suck and therefore the suction that is necessary for breastfeeding may not be adequate. Nevertheless, allowing these children to attempt breastfeeding seems to be the best strategy [6]. Because breast tissue is more flexible compared to bottles, allowing some sealing of the communication between cavities, breastfeeding may be possible.
However, breastfeeding should be avoided in syndromic patients, those with associated malformations or other severe conditions, and also patients with neurologic complications. Infants with a soft prolabium may experience a prolabium fracture during breastfeeding. These children are candidates to alternative feeding techniques such as the use of bottles and cups.
Related posts:
 Congenital Subcutaneous Mixed Venous-Lymphatic Orofacial Malformation Associated with Macroglossia: Prenatal Diagnosis with Ultrasound and Fetal MRI
Congenital Subcutaneous Mixed Venous-Lymphatic Orofacial Malformation Associated with Macroglossia: Prenatal Diagnosis with Ultrasound and Fetal MRI
 The Genetics of Facial Cleft
The Genetics of Facial Cleft
 Acromelic Frontonasal Dysplasia (Median Cleft Face Syndrome)
Acromelic Frontonasal Dysplasia (Median Cleft Face Syndrome)
 The Fetal Brain in Fetuses with Orofacial Abnormalities
The Fetal Brain in Fetuses with Orofacial Abnormalities
 Magnetic Resonance Imaging (MRI) in the Evaluation of the Fetal Face
Magnetic Resonance Imaging (MRI) in the Evaluation of the Fetal Face
 The Role of 2D/3D/4D Ultrasound in the Prenatal Assessment of Cleft Lip and Palate
The Role of 2D/3D/4D Ultrasound in the Prenatal Assessment of Cleft Lip and Palate
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


